

Age density patterns in patients medical conditions: A clustering approach
- PMID: 29944648
- PMCID: PMC6037375
- DOI: 10.1371/journal.pcbi.1006115
Age density patterns in patients medical conditions: A clustering approach
Abstract
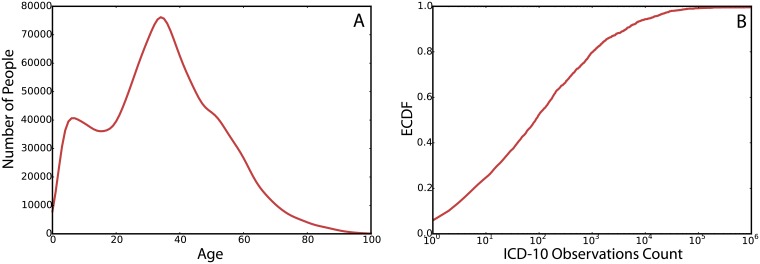
This paper presents a data analysis framework to uncover relationships between health conditions, age and sex for a large population of patients. We study a massive heterogeneous sample of 1.7 million patients in Brazil, containing 47 million of health records with detailed medical conditions for visits to medical facilities for a period of 17 months. The findings suggest that medical conditions can be grouped into clusters that share very distinctive densities in the ages of the patients. For each cluster, we further present the ICD-10 chapters within it. Finally, we relate the findings to comorbidity networks, uncovering the relation of the discovered clusters of age densities to comorbidity networks literature.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures







References
-
- Murray SA, Kendall M, Boyd K, Sheikh A. Illness trajectories and palliative care. Int Perspect Public Health Palliat Care. 2012;30:2017–19.
-
- Camilo O, Goldstein LB. Seizures and epilepsy after ischemic stroke. Stroke. 2004;35(7):1769–1775. doi: 10.1161/01.STR.0000130989.17100.96 - DOI - PubMed
-
- Murtagh FE, Murphy E, Sheerin NS. Illness trajectories: an important concept in the management of kidney failure. Nephrology Dialysis Transplantation. 2008;23(12):3746–3748. doi: 10.1093/ndt/gfn532 - DOI - PubMed
-
- Teno JM, Weitzen S, Fennell ML, Mor V. Dying trajectory in the last year of life: does cancer trajectory fit other diseases? Journal of palliative medicine. 2001;4(4):457–464. doi: 10.1089/109662101753381593 - DOI - PubMed
-
- Finkelstein J, Cha E, Scharf SM. Chronic obstructive pulmonary disease as an independent risk factor for cardiovascular morbidity. International journal of chronic obstructive pulmonary disease. 2009;4:337 doi: 10.2147/COPD.S6400 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
