

Implementation of preemptive fluid strategy as a bundle to prevent fluid overload in children with acute respiratory distress syndrome and sepsis
- PMID: 29945586
- PMCID: PMC6020419
- DOI: 10.1186/s12887-018-1188-6
Implementation of preemptive fluid strategy as a bundle to prevent fluid overload in children with acute respiratory distress syndrome and sepsis
Abstract
Background: Fluid overload (FO) is associated with unfavorable outcomes in critically ill children. Clinicians are encouraged to avoid FO; however, strategies to avoid FO are not well-described in pediatrics. Our aim was to implement a bundle strategy to prevent FO in children with sepsis and pARDS and to compare the outcomes with a historical cohort.
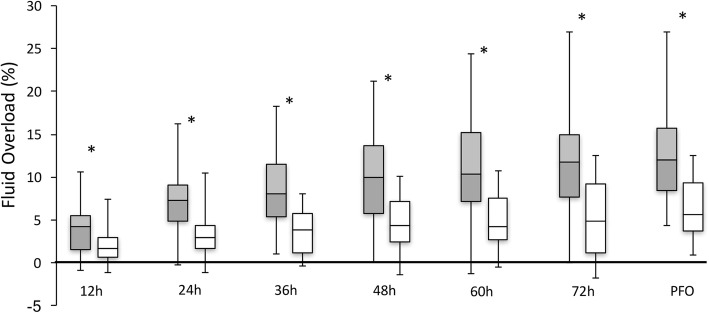
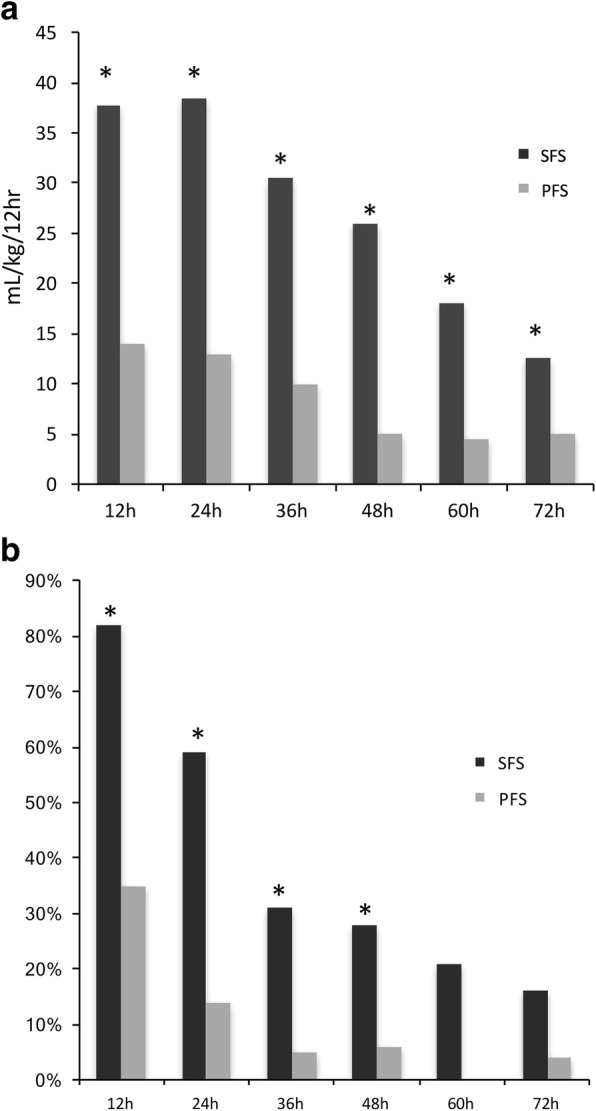
Methods: A quality improvement initiative, known as preemptive fluid strategy (PFS) was implemented to prevent early FO, in a 12-bed general PICU. Infants on mechanical ventilation (MV) fulfilling pARDS and sepsis criteria were prospectively recruited. For comparison, data from a historical cohort from 2015, with the same inclusion and exclusion criteria, was retrospectively reviewed. The PFS bundle consisted of 1. maintenance of intravenous fluids (MIVF) at 50% of requirements; 2. drug volume reduction; 3. dynamic monitoring of preload markers to determine the need for fluid bolus administration; 4. early use of diuretics; and 5. early initiation of enteral feeds. The historical cohort treatment, the standard fluid strategy (SFS), were based on physician preferences. Peak fluid overload (PFO) was the primary outcome. PFO was defined as the highest FO during the first 72 h. FO was calculated as (cumulative fluid input - cumulative output)/kg*100. Fluid input/output were registered every 12 h for 72 h.
Results: Thirty-seven patients were included in the PFS group (54% male, 6 mo (IQR 2,11)) and 39 with SFS (64%male, 3 mo (IQR1,7)). PFO was lower in PFS (6.31% [IQR4.4-10]) compared to SFS (12% [IQR8.4-15.8]). FO was lower in PFS compared to CFS as early as 12 h after admission [2.4(1.4,3.7) v/s 4.3(1.5,5.5), p < 0.01] and maintained during the study. These differences were due to less fluid input (MIVF and fluid boluses). There were no differences in the renal function test. PRBC requirements were lower during the first 24 h in the PFS (5%) compared to SFS (28%, p < 0.05). MV duration was 81 h (58,98) in PFS and 118 h (85154) in SFS(p < 0.05). PICU LOS in PFS was 5 (4, 7) and in SFS was 8 (6, 10) days.
Conclusion: Implementation of a bundle to prevent FO in children on MV with pARDS and sepsis resulted in less PFO. We observed a decrease in MV duration and PICU LOS. Future studies are needed to address if PFS might have a positive impact on health outcomes.
Keywords: Fluid overload; Mechanical ventilation; PARDS; Pediatrics; Sepsis.
Conflict of interest statement
Competing interest
The authors declare that they have no competing interests.
Ethics approval and consent to participate
Hospital Padre Hurtado’s review board approved the quality improvement project waiving the requirement for individual written consent.
Consent for publication
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Fluid overload and outcomes in critically ill children: A single center prospective cohort study.J Crit Care. 2017 Jun;39:209-213. doi: 10.1016/j.jcrc.2017.02.023. Epub 2017 Feb 16. J Crit Care. 2017. PMID: 28254390
-
Fluid overload in children with pediatric acute respiratory distress syndrome: A retrospective cohort study.Pediatr Pulmonol. 2022 Jan;57(1):300-307. doi: 10.1002/ppul.25720. Epub 2021 Oct 14. Pediatr Pulmonol. 2022. PMID: 34633156
-
Early Fluid Overload Prolongs Mechanical Ventilation in Children With Viral-Lower Respiratory Tract Disease.Pediatr Crit Care Med. 2017 Mar;18(3):e106-e111. doi: 10.1097/PCC.0000000000001060. Pediatr Crit Care Med. 2017. PMID: 28107266
-
Association between fluid overload and mortality in children with sepsis: a systematic review and meta-analysis.BMJ Paediatr Open. 2023 Nov;7(1):e002094. doi: 10.1136/bmjpo-2023-002094. BMJ Paediatr Open. 2023. PMID: 37989355 Free PMC article.
-
Fluid Overload.Crit Care Clin. 2015 Oct;31(4):803-21. doi: 10.1016/j.ccc.2015.06.013. Epub 2015 Jul 29. Crit Care Clin. 2015. PMID: 26410146 Review.
Cited by
-
Reducing NICU ventilator days by preventing fluid overload with the CAN-U-P-LOTS standardized bundle.Pediatr Res. 2025 Jul 11. doi: 10.1038/s41390-025-04078-x. Online ahead of print. Pediatr Res. 2025. PMID: 40646283
-
Fluid overload: clinical outcomes in pediatric intensive care unit.J Pediatr (Rio J). 2023 May-Jun;99(3):241-246. doi: 10.1016/j.jped.2022.10.002. Epub 2022 Nov 10. J Pediatr (Rio J). 2023. PMID: 36370749 Free PMC article.
-
ESPNIC clinical practice guidelines: intravenous maintenance fluid therapy in acute and critically ill children- a systematic review and meta-analysis.Intensive Care Med. 2022 Dec;48(12):1691-1708. doi: 10.1007/s00134-022-06882-z. Epub 2022 Oct 26. Intensive Care Med. 2022. PMID: 36289081 Free PMC article.
-
Care bundles for improving outcomes in patients with COVID-19 or related conditions in intensive care - a rapid scoping review.Cochrane Database Syst Rev. 2020 Dec 21;12(12):CD013819. doi: 10.1002/14651858.CD013819. Cochrane Database Syst Rev. 2020. PMID: 33348427 Free PMC article.
-
Analysis of surgical mortality in rural South Australia: a review of four major rural hospital in South Australia.ANZ J Surg. 2022 Jul;92(7-8):1681-1691. doi: 10.1111/ans.17833. Epub 2022 Jun 8. ANZ J Surg. 2022. PMID: 35674399 Free PMC article. Review.
References
-
- Oliveira CF, Nogueira de Sá FR, Oliveira DS, Gottschald AF, Moura JD, Shibata AR, Troster EJ, Vaz FA, Carcillo JA. Time- and fluid-sensitive resuscitation for hemodynamic support of children in septic shock: barriers to the implementationof the American College of Critical Care Medicine/Pediatric Advanced Life Support Guidelines in a pediatric intensive care unit in a developing world. Pediatr Emerg Care. 2008;24(12):810–815. doi: 10.1097/PEC.0b013e31818e9f3a. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
