

Different latent class models were used and evaluated for assessing the accuracy of campylobacter diagnostic tests: overcoming imperfect reference standards?
- PMID: 29945689
- PMCID: PMC6090718
- DOI: 10.1017/S0950268818001723
Different latent class models were used and evaluated for assessing the accuracy of campylobacter diagnostic tests: overcoming imperfect reference standards?
Abstract
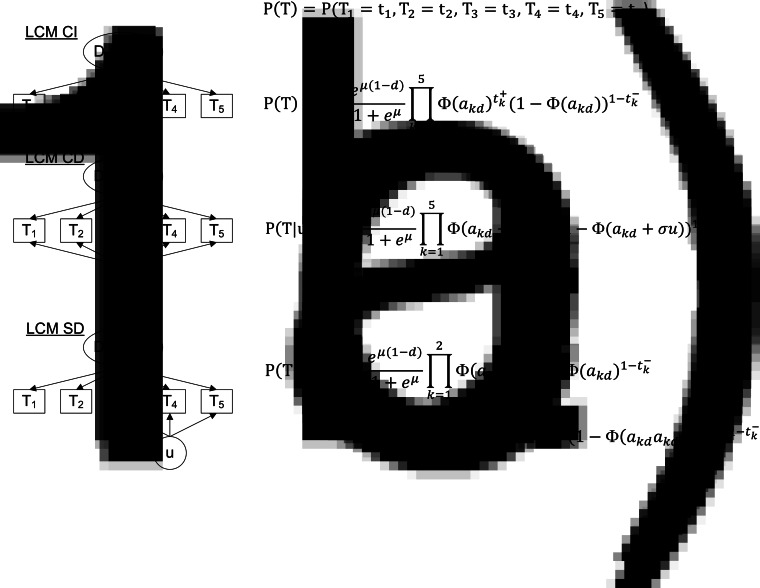
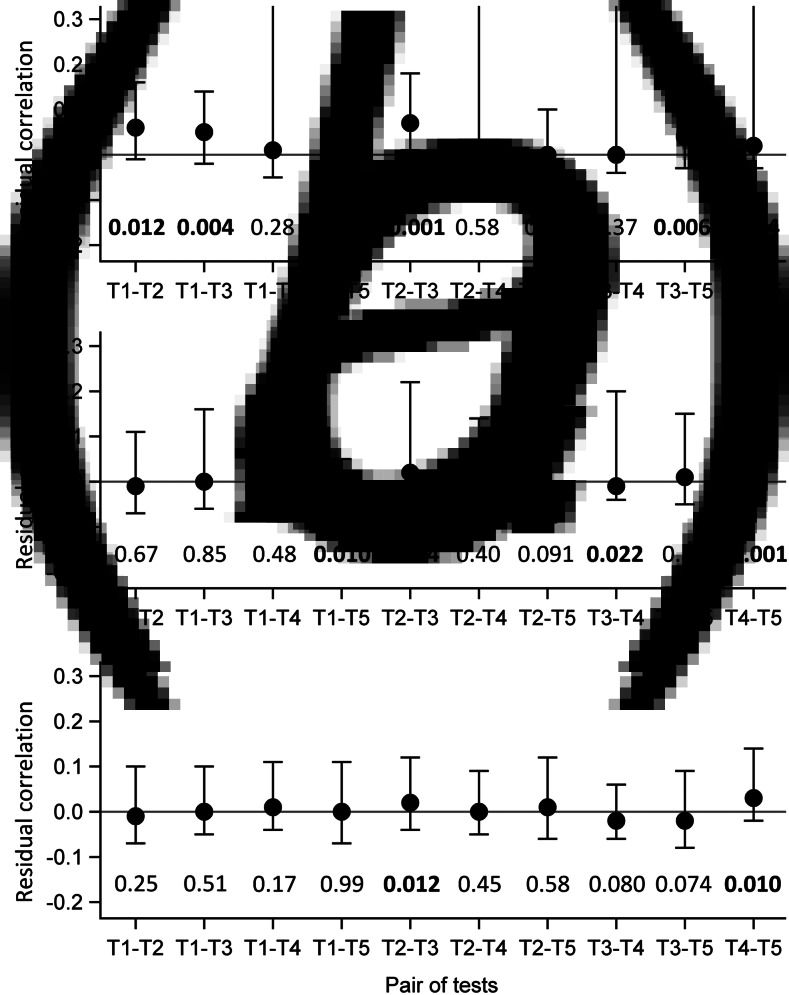
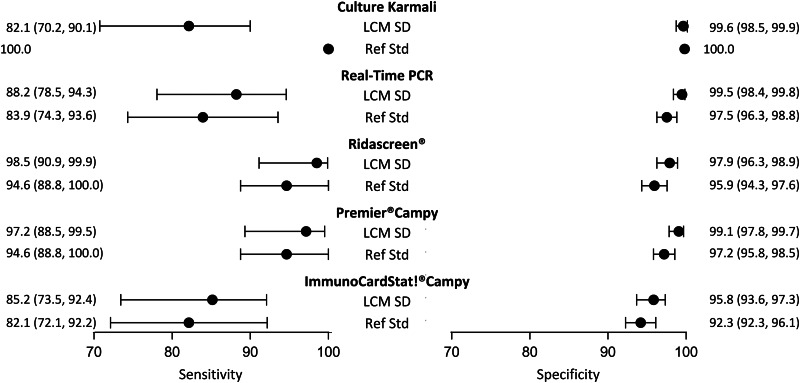
In the absence of perfect reference standard, classical techniques result in biased diagnostic accuracy and prevalence estimates. By statistically defining the true disease status, latent class models (LCM) constitute a promising alternative. However, LCM is a complex method which relies on parametric assumptions, including usually a conditional independence between tests and might suffer from data sparseness. We carefully applied LCMs to assess new campylobacter infection detection tests for which bacteriological culture is an imperfect reference standard. Five diagnostic tests (culture, polymerase chain reaction and three immunoenzymatic tests) of campylobacter infection were collected in 623 patients from Bordeaux and Lyon Hospitals, France. Their diagnostic accuracy were estimated with standard and extended LCMs with a thorough examination of models goodness-of-fit. The model including a residual dependence specific to the immunoenzymatic tests best complied with LCM assumptions. Asymptotic results of goodness-of-fit statistics were substantially impaired by data sparseness and empirical distributions were preferred. Results confirmed moderate sensitivity of the culture and high performances of immunoenzymatic tests. LCMs can be used to estimate diagnostic tests accuracy in the absence of perfect reference standard. However, their implementation and assessment require specific attention due to data sparseness and limitations of existing software.
Keywords: Campylobacter; diagnostic accuracy; imperfect gold standard; latent class model; sparseness.
Conflict of interest statement
None.
Figures
Similar articles
-
Problems in detecting misfit of latent class models in diagnostic research without a gold standard were shown.J Clin Epidemiol. 2016 Jun;74:158-66. doi: 10.1016/j.jclinepi.2015.11.012. Epub 2015 Nov 25. J Clin Epidemiol. 2016. PMID: 26628335
-
STARD-BLCM: Standards for the Reporting of Diagnostic accuracy studies that use Bayesian Latent Class Models.Prev Vet Med. 2017 Mar 1;138:37-47. doi: 10.1016/j.prevetmed.2017.01.006. Epub 2017 Jan 12. Prev Vet Med. 2017. PMID: 28237234
-
Evaluation of the Diagnostic Accuracy of Two Immunochromatographic Tests Detecting Campylobacter in Stools and Their Role in Campylobacter Infection Diagnosis.J Clin Microbiol. 2018 Mar 26;56(4):e01567-17. doi: 10.1128/JCM.01567-17. Print 2018 Apr. J Clin Microbiol. 2018. PMID: 29436423 Free PMC article.
-
Estimation of diagnostic test accuracy without full verification: a review of latent class methods.Stat Med. 2014 Oct 30;33(24):4141-69. doi: 10.1002/sim.6218. Epub 2014 Jun 9. Stat Med. 2014. PMID: 24910172 Free PMC article. Review.
-
Bayesian meta-analysis of diagnostic tests allowing for imperfect reference standards.Stat Med. 2013 Dec 30;32(30):5398-413. doi: 10.1002/sim.5959. Epub 2013 Sep 4. Stat Med. 2013. PMID: 24003003 Review.
Cited by
-
Evaluation of CAMPYLOBACTER QUIK CHEK™ rapid membrane enzyme immunoassay to detect Campylobacter spp. antigen in stool samples.Gut Pathog. 2021 Jan 22;13(1):4. doi: 10.1186/s13099-021-00400-0. Gut Pathog. 2021. PMID: 33482881 Free PMC article.
-
Determining antenatal medicine exposures in South African women: a comparison of three methods of ascertainment.BMC Pregnancy Childbirth. 2022 Jun 3;22(1):466. doi: 10.1186/s12884-022-04765-1. BMC Pregnancy Childbirth. 2022. PMID: 35658841 Free PMC article.
-
Detecting departures from the conditional independence assumption in diagnostic latent class models: a simulation study.BMC Med Res Methodol. 2024 Dec 5;24(1):299. doi: 10.1186/s12874-024-02432-x. BMC Med Res Methodol. 2024. PMID: 39639189 Free PMC article.
-
Comparative diagnostic accuracy studies with an imperfect reference standard - a comparison of correction methods.BMC Med Res Methodol. 2021 Apr 12;21(1):67. doi: 10.1186/s12874-021-01255-4. BMC Med Res Methodol. 2021. PMID: 33845775 Free PMC article.
-
Stool DNA testing for early detection of colorectal cancer: systematic review using the HTA Core Model® for Rapid Relative Effectiveness Assessment.Ger Med Sci. 2023 Jun 23;21:Doc06. doi: 10.3205/000320. eCollection 2023. Ger Med Sci. 2023. PMID: 37426885 Free PMC article.
References
-
- Valenstein PN (1990) Evaluating diagnostic tests with imperfect standards. American Journal of Clinical Pathology 93, 252–258. - PubMed
-
- Ihorst G et al. (2007) The use of imperfect diagnostic tests had an impact on prevalence estimation. Journal of Clinical Epidemiology 60, 902–910. - PubMed
-
- Rutjes AWS et al. (2007) Evaluation of diagnostic tests when there is no gold standard. A review of methods. Health Technology Assessment 11, iii, ix-51. - PubMed
-
- Reitsma JB et al. (2009) A review of solutions for diagnostic accuracy studies with an imperfect or missing reference standard. Journal of Clinical Epidemiology 62, 797–806. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
