

High Burden of 30-Day Readmissions After Acute Venous Thromboembolism in the United States
- PMID: 29945913
- PMCID: PMC6064903
- DOI: 10.1161/JAHA.118.009047
High Burden of 30-Day Readmissions After Acute Venous Thromboembolism in the United States
Abstract
Background: Venous thromboembolism (VTE) is the third leading cause of vascular disease and accounts for $10 billion in annual US healthcare costs. The nationwide burden of 30-day readmissions after such events has not been comprehensively assessed.
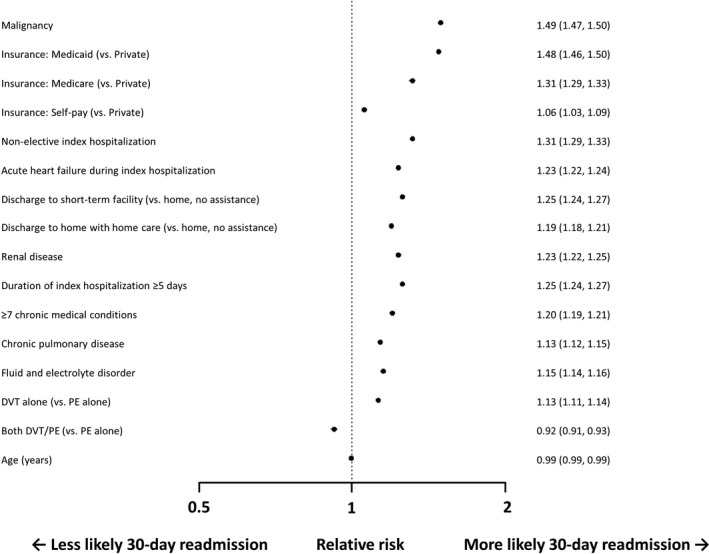
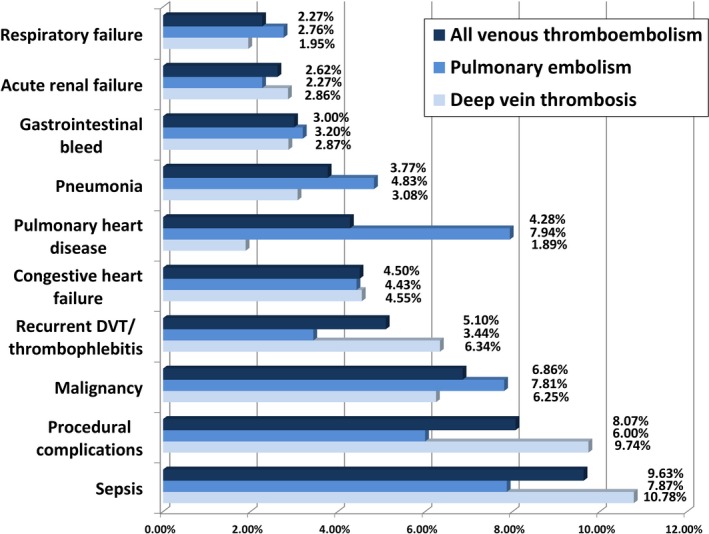
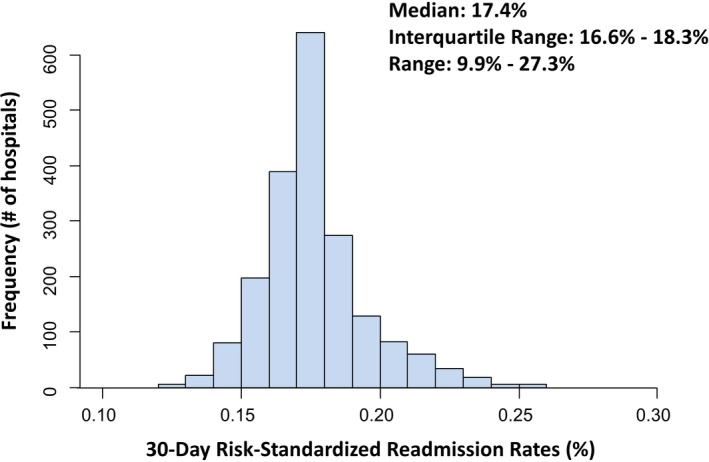
Methods and results: We analyzed adults ≥18 years of age with hospitalizations associated with acute VTE between January 1, 2010, and December 31, 2014, in the Nationwide Readmissions Database. International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) codes were used to identify hospitalizations associated with acute pulmonary embolism or deep vein thrombosis. The primary outcome was the rate of unplanned 30-day readmission. Hierarchical logistic regression was used to calculate hospital-specific 30-day risk-standardized readmission rates, a marker of healthcare quality. Among 1 176 335 hospitalizations with acute VTE, in-hospital death occurred in 6.2%. VTE was associated with malignancy in 19.7%, recent surgery in 19.3%, recent trauma in 4.6%, hypercoagulability in 3.3%, and pregnancy in 1.0%. Among survivors to discharge, the 30-day readmission rate was 17.5%, with no significant difference in rates across study years (17.4%-17.7%; P=0.10 for trend). Major predictors of readmission were malignancy (relative risk, 1.49, 95% confidence interval 1.47-1.50), Medicaid insurance (relative risk, 1.48, 95% confidence interval 1.46-1.50), and nonelective index admission (relative risk, 1.31, 95% confidence interval 1.29-1.33). Top causes of readmission included sepsis (9.6%) and procedural complications (8.1%). Median rehospitalization costs were $9781.7 (interquartile range, $5430.7-$18 784.1), and 8.1% died during readmission. The interquartile range in risk-standardized readmission rates was 16.6% to 18.3%, suggesting modest interhospital heterogeneity in readmission risk.
Conclusions: Nearly 1 in 5 patients with acute VTE were readmitted within 30 days. Predictors and causes of readmission were primarily related to patient characteristics and complications from comorbid conditions, whereas healthcare quality had a moderate impact on readmission risk.
Keywords: deep vein thrombosis; pulmonary embolism; readmission; venous thromboembolism.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Raskob GE, Angchaisuksiri P, Blanco AN, Buller H, Gallus A, Hunt BJ, Hylek EM, Kakkar A, Konstantinides SV, McCumber M. Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol. 2014;34:2363–2371. - PubMed
-
- Silverstein MD, Heit JA, Mohr DN, Petterson TM, O'fallon WM, Melton LJ. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25‐year population‐based study. Arch Intern Med. 1998;158:585–593. - PubMed
-
- Weller WE, Gallagher BK, Cen L, Hannan EL. Readmissions for venous thromboembolism: expanding the definition of patient safety indicators. Jt Comm J Qual Saf. 2004;30:497–504. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
