

Risankizumab, an IL-23 inhibitor, for ankylosing spondylitis: results of a randomised, double-blind, placebo-controlled, proof-of-concept, dose-finding phase 2 study
- PMID: 29945918
- PMCID: PMC6104676
- DOI: 10.1136/annrheumdis-2018-213328
Risankizumab, an IL-23 inhibitor, for ankylosing spondylitis: results of a randomised, double-blind, placebo-controlled, proof-of-concept, dose-finding phase 2 study
Abstract
Objectives: To evaluate the efficacy and safety of risankizumab, a humanised monoclonal antibody targeting the p19 subunit of interleukin-23 (IL-23), in patients with active ankylosing spondylitis (AS).
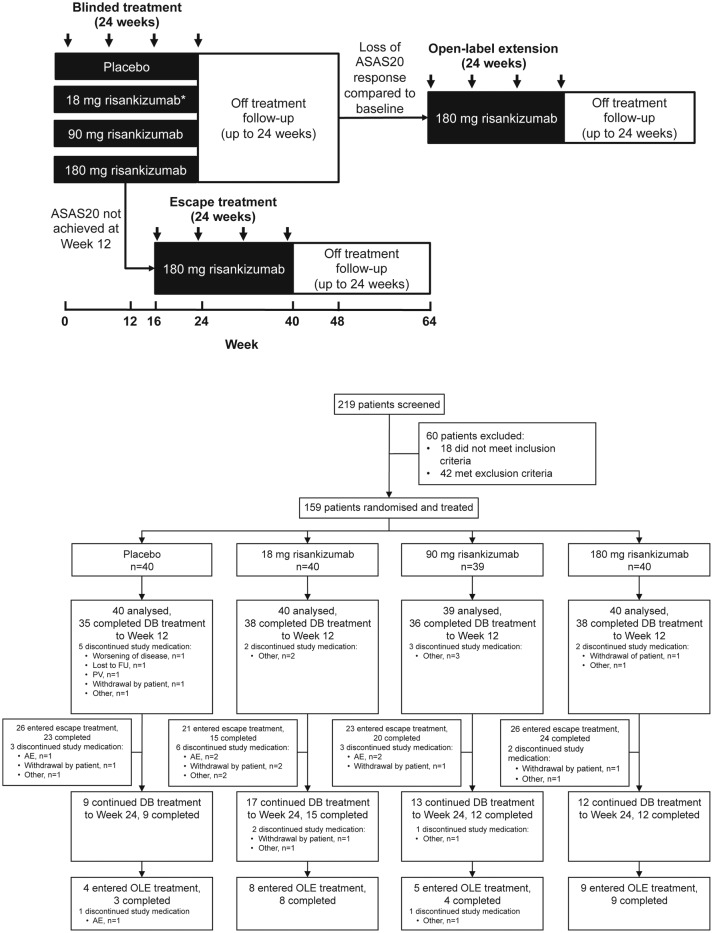
Methods: A total of 159 patients with biological-naïve AS, with active disease (Bath Ankylosing Spondylitis Disease Activity Index score of ≥4), were randomised (1:1:1:1) to risankizumab (18 mg single dose, 90 mg or 180 mg at day 1 and weeks 8, 16 and 24) or placebo over a 24-week blinded period. The primary outcome was a 40% improvement in Assessment in Spondylo Arthritis International Society (ASAS40) at week 12. Safety was assessed in patients who received at least one dose of study drug.
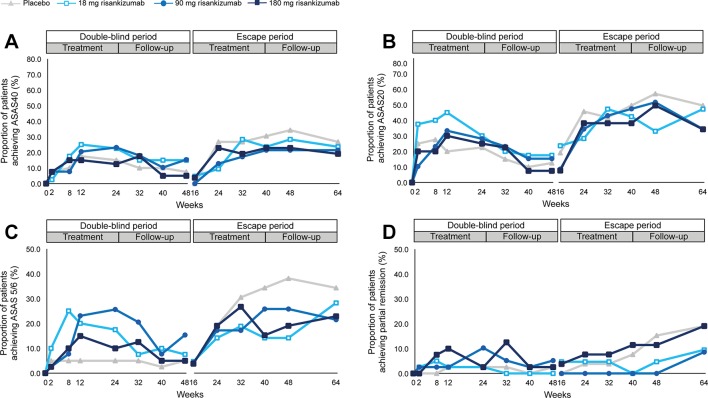
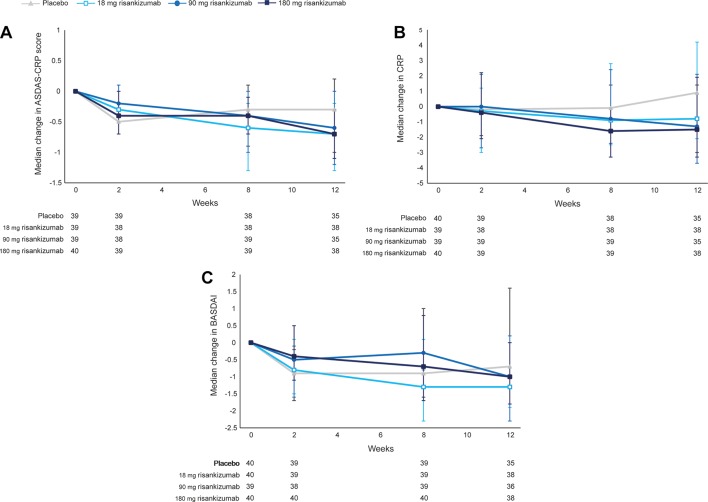
Results: At week 12, ASAS40 response rates were 25.5%, 20.5% and 15.0% in the 18 mg, 90 mg and 180 mg risankizumab groups, respectively, compared with 17.5% in the placebo group. The estimated difference in proportion between the 180 mg risankizumab and placebo groups (primary endpoint) was -2.5% (95% CI -21.8 to 17.0; p=0.42). Rates of adverse events were similar in all treatment groups.
Conclusions: Treatment with risankizumab did not meet the study primary endpoint and showed no evidence of clinically meaningful improvements compared with placebo in patients with active AS, suggesting that IL-23 may not be a relevant driver of disease pathogenesis and symptoms in AS.
Trial registration number: NCT02047110; Pre-results.
Keywords: DMARDs (biologic); ankylosing spondylitis; treatment.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: DB reports grants from AbbVie, Pfizer, UCB, MSD, Novartis and Eli Lilly and part-time employment at UCB. MØ reports grants, personal fees and non-financial support from AbbVie, BMS, Merck, UCB and Novartis; grants and personal fees from Celgene; personal fees and non-financial support from Janssen, Pfizer and Roche; and personal fees from Boehringer Ingelheim, Eli Lilly, Sanofi, Regeneron, Orion and Hospira. JS reports personal fees from Boehringer Ingelheim, AbbVie, Janssen, Lilly, Merck, Novartis, Pfizer and UCB. PJ reports grants from AbbVie, Daiichi Sankyo, Boehringer Ingelheim, Lilly, Novartis, Roche and UCB and grants and personal fees from BMS and Pfizer. YD, CP, SV, DBH, SA, PS and SJP report being employees of Boehringer Ingelheim.
Figures
References
-
- Ward MM, Deodhar A, Akl EA, et al. American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network 2015 Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis. Arthritis Rheumatol 2016;68:282–98. 10.1002/art.39298 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
