

Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group
- PMID: 29946347
- PMCID: PMC6006983
- DOI: 10.1186/s13017-018-0185-2
Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group
Abstract
Background: Adhesive small bowel obstruction (ASBO) is a common surgical emergency, causing high morbidity and even some mortality. The adhesions causing such bowel obstructions are typically the footprints of previous abdominal surgical procedures. The present paper presents a revised version of the Bologna guidelines to evidence-based diagnosis and treatment of ASBO. The working group has added paragraphs on prevention of ASBO and special patient groups.
Methods: The guideline was written under the auspices of the World Society of Emergency Surgery by the ASBO working group. A systematic literature search was performed prior to the update of the guidelines to identify relevant new papers on epidemiology, diagnosis, and treatment of ASBO. Literature was critically appraised according to an evidence-based guideline development method. Final recommendations were approved by the workgroup, taking into account the level of evidence of the conclusion.
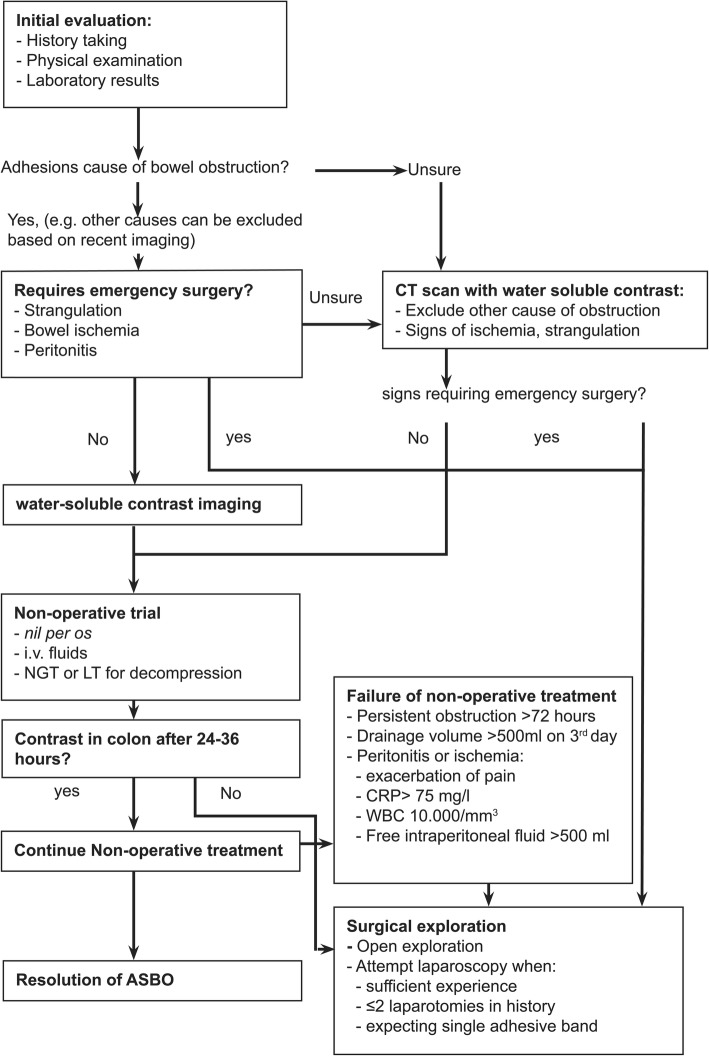
Recommendations: Adhesion formation might be reduced by minimally invasive surgical techniques and the use of adhesion barriers. Non-operative treatment is effective in most patients with ASBO. Contraindications for non-operative treatment include peritonitis, strangulation, and ischemia. When the adhesive etiology of obstruction is unsure, or when contraindications for non-operative management might be present, CT is the diagnostic technique of choice. The principles of non-operative treatment are nil per os, naso-gastric, or long-tube decompression, and intravenous supplementation with fluids and electrolytes. When operative treatment is required, a laparoscopic approach may be beneficial for selected cases of simple ASBO.Younger patients have a higher lifetime risk for recurrent ASBO and might therefore benefit from application of adhesion barriers as both primary and secondary prevention.
Discussion: This guideline presents recommendations that can be used by surgeons who treat patients with ASBO. Scientific evidence for some aspects of ASBO management is scarce, in particular aspects relating to special patient groups. Results of a randomized trial of laparoscopic versus open surgery for ASBO are awaited.
Keywords: Adhesions; Laparoscopy; Laparotomy; Small bowel obstruction; Surgery.
Conflict of interest statement
Not applicableThe authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- NELA Project Team . The second patient report of the National Emergency Laparotomy Audit (NELA) London: The Royal College of Anaesthetists; 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
