

Clinical agreement in the American Society of Anesthesiologists physical status classification
- PMID: 29946447
- PMCID: PMC6008948
- DOI: 10.1186/s13741-018-0094-7
Clinical agreement in the American Society of Anesthesiologists physical status classification
Abstract
Background: The American Society of Anesthesiologists physical status (ASA-PS) classification is not intended to predict risk, but increasing ASA-PS class has been associated with increased perioperative mortality. The ASA-PS class is being used by many institutions to identify patients that may require further workup or exams preoperatively. Studies regarding the ASA-PS classification system show significant variability in class assignment by anesthesiologists as well as providers of different specialties when provided with short clinical scenarios. Discrepancies in the ASA-PS accuracy have the potential to lead to unnecessary testing and cancelation of surgical procedures. Our study aimed to determine whether these differences in ASA-PS classification were present when actual patients were evaluated rather than previously published scenario-based studies.
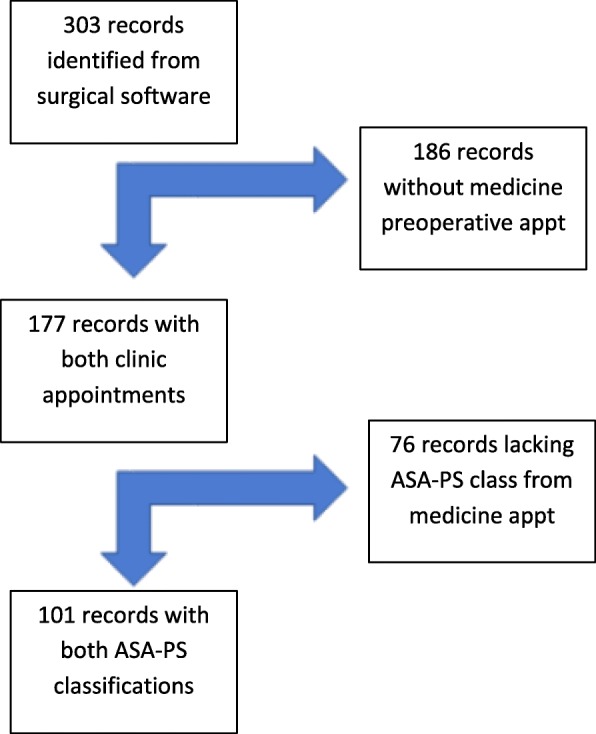
Methods: A retrospective chart review was completed for patients >/= 65 years of age undergoing elective total hip or total knee replacements. One hundred seventy-seven records were reviewed of which 101 records had the necessary data. The outcome measures noted were the ASA-PS classification assigned by the internal medicine clinic provider, the ASA-PS classification assigned by the Pre-Anesthesia Unit (PAU) clinic provider, and the ASA-PS classification assigned on the day of surgery (DOS) by the anesthesia provider conducting the anesthetic care.
Results: A statistically significant difference was shown between the internal medicine and the PAU preoperative ASA-PS designation as well as between the internal medicine and DOS designation (McNemar p = 0.034 and p = 0.025). Low kappa values were obtained confirming the inter-observer variation in the application of the ASA-PS classification of patients by providers of different specialties [Kappa of 0.170 (- 0.001, 0.340) and 0.156 (- 0.015, 0.327)].
Conclusions: There was disagreement in the ASA-PS class designation between two providers of different specialties when evaluating the same patients with access to full medical records. When the anesthesia-run PAU and the anesthesia assigned DOS ASA-PS class designations were evaluated, there was agreement. This agreement was seen between anesthesia providers regardless of education or training level. The difference in the application of the ASA-PS classification in our study appeared to be reflective of department membership and not reflective of the individual provider's level of training.
Keywords: Anesthesiology/standards; Preoperative care; Risk assessment/classification; Variation between specialties.
Conflict of interest statement
Approved by Institutional IRB, ref. c.2017.078e.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- Cuvillon P, Nouvellon E, Marret E, Albaladejo P, Fortier LP, Fabbro-Perray P, et al. American Society of Anesthesiologists’ physical status system: a multicentre Francophone study to analyse reasons for classification disagreement. Eur J Anaesthesiol. 2011;28:742–747. doi: 10.1097/EJA.0b013e328348fc9d. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
