

Outcomes and Treatment Options for Duodenal Adenocarcinoma: A Systematic Review and Meta-Analysis
- PMID: 29946997
- PMCID: PMC6097725
- DOI: 10.1245/s10434-018-6567-6
Outcomes and Treatment Options for Duodenal Adenocarcinoma: A Systematic Review and Meta-Analysis
Abstract
Background: Duodenal adenocarcinoma (DA) is a rare tumor for which survival data per treatment modality and disease stage are unclear. This systematic review and meta-analysis aims to summarize the current literature on patient outcome after surgical, (neo)adjuvant, and palliative treatment in patients with DA.
Methods: A systematic search was performed according to the preferred reporting items for systematic reviews and meta-analyses guidelines, to 25 April 2017. Primary outcome was overall survival (OS), specified for treatment strategy or disease stage. Random-effects models were used for the calculation of pooled odds ratios per treatment modality. Included papers were also screened for prognostic factors.
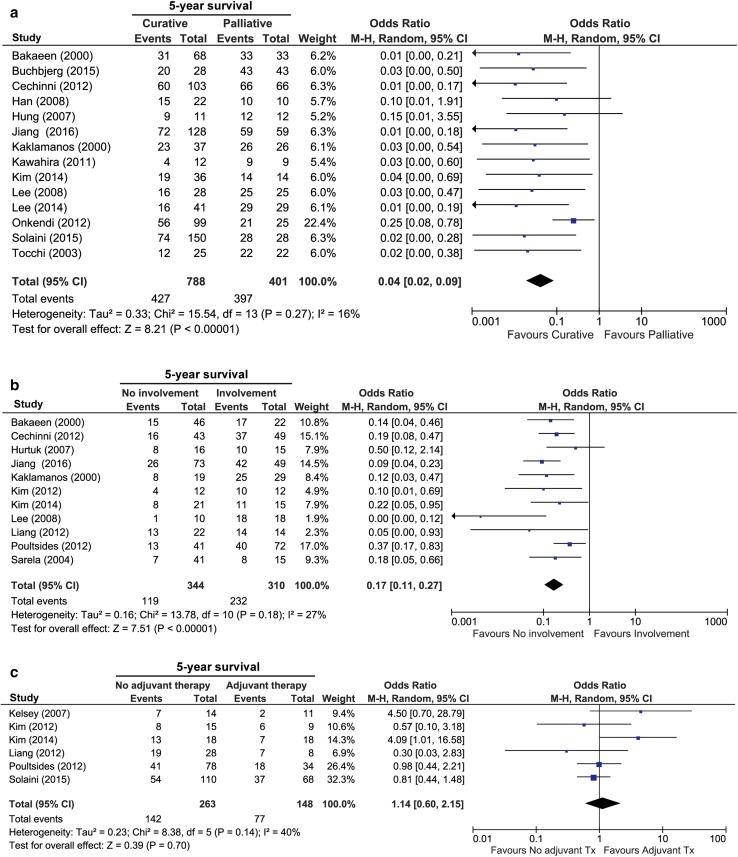
Results: A total of 26 observational studies, comprising 6438 patients with DA, were included. Of these, resection with curative intent was performed in 71% (range 53-100%) of patients, and 29% received palliative treatment (range 0-61%). The pooled 5-year OS rate was 46% after curative resection, compared with 1% in palliative-treated patients (OR 0.04, 95% confidence interval [CI] 0.02-0.09, p < 0.0001). Both segmental resection and pancreaticoduodenectomy allowed adequate assessment of lymph node involvement and resulted in similar OS. Lymph node involvement correlated with worse OS (pooled 5-year survival rate 21% for nodal metastases vs. 65% for node-negative disease; OR 0.17, 95% CI 0.11-0.27, p < 0.0001). In the current literature, no survival benefit for adjuvant therapy after curative resection was found.
Conclusion: Resection with curative intent, either pancreaticoduodenectomy or segmental resection, and lack of nodal metastases, favors survival for DA. Further studies exploring multimodality (neo)adjuvant therapy are warranted to investigate their benefit.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Comment in
-
ASO Author Reflections: Current Treatment Options for Duodenal Adenocarcinoma-A Call for Collaborative Studies.Ann Surg Oncol. 2018 Dec;25(Suppl 3):737-738. doi: 10.1245/s10434-018-6896-5. Epub 2018 Oct 16. Ann Surg Oncol. 2018. PMID: 30327972 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
