

High risk breast lesions identified on MRI-guided vacuum-assisted needle biopsy: outcome of surgical excision and imaging follow-up
- PMID: 29947265
- PMCID: PMC6350470
- DOI: 10.1259/bjr.20180300
High risk breast lesions identified on MRI-guided vacuum-assisted needle biopsy: outcome of surgical excision and imaging follow-up
Abstract
Objective:: To determine whether breast MRI-guided vacuum-assisted biopsy (MRI-VAB) high-risk lesion histology influences surgical or long-term imaging follow-up outcomes.
Methods:: Patients with imaging-concordant high-risk findings on 9-gauge breast MRI-VAB between January 2007 and July 2012 who had surgical histopathology or 2 year imaging follow-up were retrospectively reviewed.
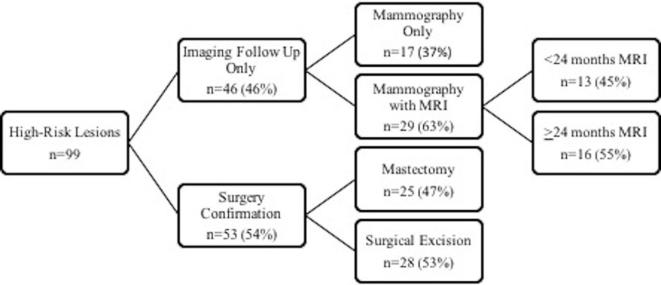
Results:: 90 patients with 99 lesions were included. Lesions were atypical ductal hyperplasia (ADH) (n = 21), lobular neoplasia [n = 36; atypical lobular hyperplasia (ALH) (n = 22), lobular carcinoma in situ (LCIS) (n = 6), and ALH plus LCIS (n = 8)], and other high-risk lesion (n = 42; papillary lesions, radial scar, flat epithelial atypia, atypia unspecified). Of 53 excised lesions, 6 (11%) were upgraded to invasive cancer or ductal carcinoma in situ (DCIS). 4 of 21 (19%) ADH lesions were upgraded to DCIS. 2 of 36 (6%) lobular neoplasia lesions, both combined ALH and LCIS, were upgraded to DCIS, and invasive lobular carcinoma, respectively. The remaining 46 lesions were managed conservatively with imaging follow-up: 17 (37%) had mammography only, while 29 (63%) had mammography and MRI follow-up. There was no evidence of breast cancer development at the site of MRI-VAB in the cases with only imaging follow-up.
Conclusion:: We conclude that the upgrade rate for high-risk lesions at MRI-VAB at surgical excision is low. Surgical excision is warranted for ADH and combined ALH-LCIS lesions. For other lesions, a multidisciplinary approach to decide on personalized management may be appropriate.
Advances in knowledge:: Surgical excision is warranted for ADH lesions and combined ALH-LCIS lesions identified at breast MRI-VAB. A multidisciplinary approach to patient management of other high-risk lesions may be appropriate.
Conflict of interest statement
Figures
Similar articles
-
High-risk lesions diagnosed at MRI-guided vacuum-assisted breast biopsy: imaging characteristics, outcome of surgical excision or imaging follow-up.Breast Cancer. 2020 May;27(3):405-414. doi: 10.1007/s12282-019-01032-8. Epub 2019 Dec 14. Breast Cancer. 2020. PMID: 31838725
-
High-Risk Lesions Detected by MRI-Guided Core Biopsy: Upgrade Rates at Surgical Excision and Implications for Management.AJR Am J Roentgenol. 2021 Mar;216(3):622-632. doi: 10.2214/AJR.20.23040. Epub 2021 Jan 13. AJR Am J Roentgenol. 2021. PMID: 33439046
-
Magnetic resonance imaging-guided core needle breast biopsies resulting in high-risk histopathologic findings: upstage frequency and lesion characteristics.Clin Breast Cancer. 2015 Jun;15(3):234-9. doi: 10.1016/j.clbc.2014.12.005. Epub 2014 Dec 24. Clin Breast Cancer. 2015. PMID: 25579460
-
The positive predictive value of vacuum assisted biopsy (VAB) in predicting final histological diagnosis for breast lesions of uncertain malignancy (B3 lesions): A systematic review & meta-analysis.Eur J Surg Oncol. 2022 Jul;48(7):1464-1474. doi: 10.1016/j.ejso.2022.04.005. Epub 2022 Apr 15. Eur J Surg Oncol. 2022. PMID: 35491362
-
[Benign proliferative breast disease with and without atypia].J Gynecol Obstet Biol Reprod (Paris). 2015 Dec;44(10):980-95. doi: 10.1016/j.jgyn.2015.09.037. Epub 2015 Nov 3. J Gynecol Obstet Biol Reprod (Paris). 2015. PMID: 26545856 Review. French.
Cited by
-
Primary Extranodal Follicular T-Cell Lymphoma and Ductal Breast Carcinoma Diagnosed by a Magnetic Resonance Imaging-Guided Vacuum-Assisted Biopsy: A Case Report.Am J Case Rep. 2021 Jul 6;22:e929309. doi: 10.12659/AJCR.929309. Am J Case Rep. 2021. PMID: 34226439 Free PMC article.
-
Radial Scar: a management dilemma.Radiol Med. 2021 Jun;126(6):774-785. doi: 10.1007/s11547-021-01344-w. Epub 2021 Mar 20. Radiol Med. 2021. PMID: 33743143 Free PMC article. Review.
-
High-risk lesions in the breast diagnosed by MRI-guided core biopsy: upgrade rates and features associated with malignancy.Breast Cancer Res Treat. 2022 Dec;196(3):517-525. doi: 10.1007/s10549-022-06761-7. Epub 2022 Oct 15. Breast Cancer Res Treat. 2022. PMID: 36242709
-
Are Columnar Cell Lesions the Earliest Non-Obligate Precursor in the Low-Grade Breast Neoplasia Pathway?Curr Oncol. 2022 Aug 11;29(8):5664-5681. doi: 10.3390/curroncol29080447. Curr Oncol. 2022. PMID: 36005185 Free PMC article. Review.
-
B3 Lesions at Vacuum-Assisted Breast Biopsy under Ultrasound or Mammography Guidance: A Single-Center Experience on 3634 Consecutive Biopsies.Cancers (Basel). 2021 Oct 29;13(21):5443. doi: 10.3390/cancers13215443. Cancers (Basel). 2021. PMID: 34771606 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
