

Review
doi: 10.1259/bjr.20170856.
Epub 2018 Jul 25.
Imaging of inguinal-related groin pain in athletes
Affiliations
- PMID: 29947268
- PMCID: PMC6319843
- DOI: 10.1259/bjr.20170856
Item in Clipboard
Review
Imaging of inguinal-related groin pain in athletes
Br J Radiol.
2018 Dec.
Abstract
Inguinal canal-related groin pain is common in athletes and may involve numerous structures such as the conjoint tendon and the transversalis fascia. Ultrasound is the only dynamic tool that shows the passage of preperitoneal fat at the level of the Hesselbach triangle and allows excluding true inguinal hernias. Fascia transversalis bulging and inguinal ring dilatation may also be described. MRI assesses injuries of rectus abdominis and adductor longus enthesis and osteitis symphysis but its accuracy for the diagnosis of inguinal-related groin pain remains debated.
Figures
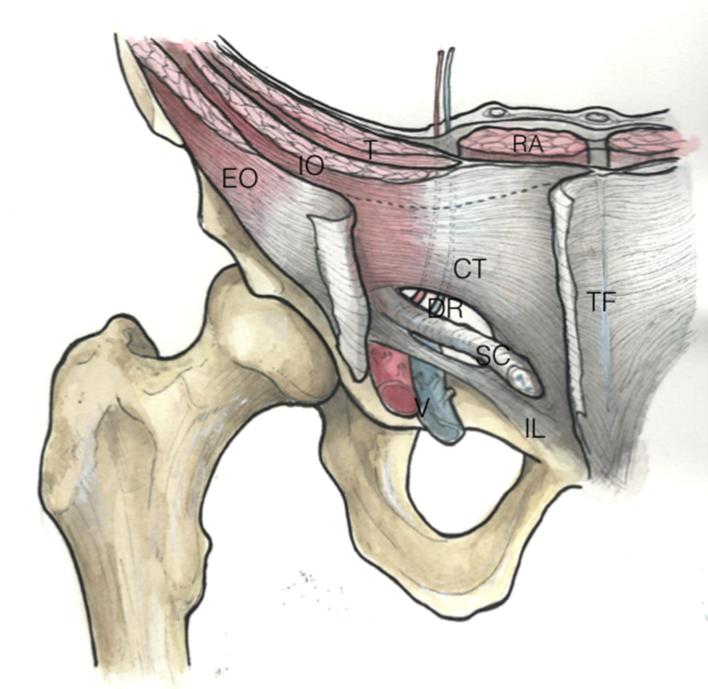
Schematic drawing from an anterior view of the inguinal canal. The internal deep ring is superior, and located at the middle of the inguinal ligament. It is inferior and mediolateral to the conjoint tendon, and lateral to the inferior epigastric vessels. The external superficial ring is a triangular opening in the external oblique aponeurosis. The inferior epigastric artery (a) and vein (v) originate from the external iliac artery and vein and lie medial to the internal inguinal ring. CT, conjoint tendon; EO, external oblique muscle; EOA, external oblique aponeurosis; IL, inguinal ligament; IO, interne oblique muscle; RA, rectus abdominis; SC, spermatic cord; T, transverse muscle; TF, transversalis fascia; DR, deep ring.
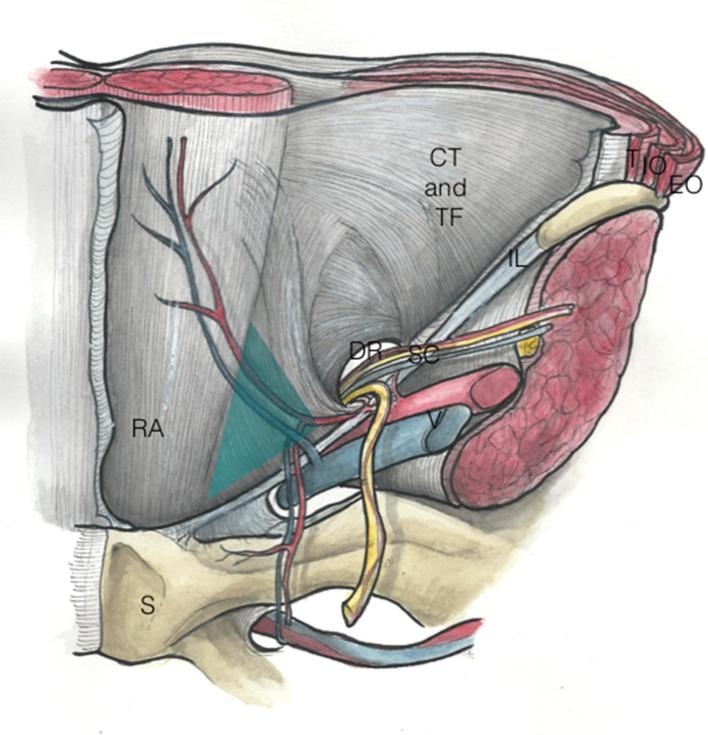
Schematic drawing from a posterior view of the Hesselbach triangle. Medial to this deep ring, the Hesselbach triangle is medial to the inferior epigastric vessels, lateral to the rectus abdominis muscles and cranial to the inguinal ligament. CT, conjoint tendon; TF, transversalis fascia; IL, inguinal ligament; RA, rectus abdominis; DR, deep ring; S, symphysis; SC, spermatic cord; T, transverse muscle; O, interne oblique muscle; E, external oblique muscle.
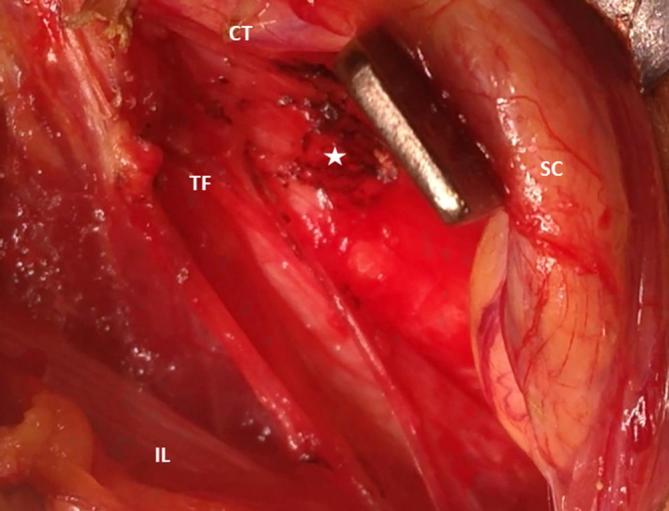
Anterior laparoscopic view of the inguinal canal during Shouldice procedure shows dehiscence of the TF and protrusion of pre-peritoneal fat (star). CT, conjoint tendon; IL, inguinal ligament; SC, Spermatic cord; TF, transversalis fascia.
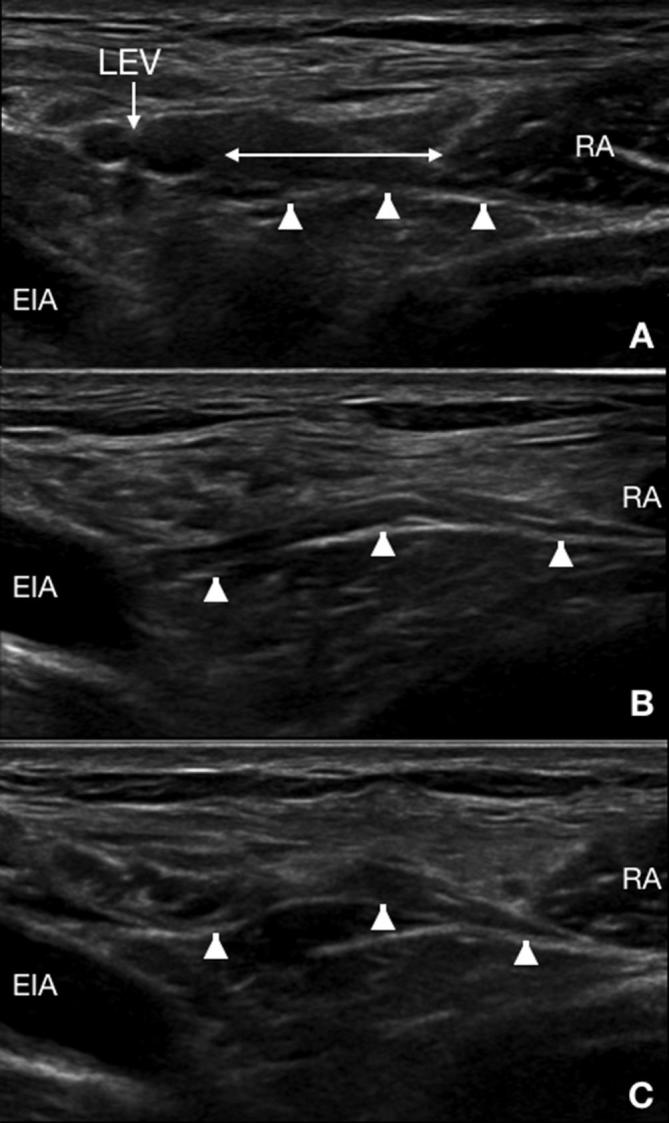
Ultrasound of an asymptomatic male athlete. Dynamic ultrasound in the axial plane at rest (A) and at the beginning (B) and end (C) of Valsalva’s maneuvers shows the location of the Hesselbach triangle (double arrows) at the level of the LEV. Additionally, there is a slight convexity of the fascia transversalis (arrowheads) without protrusion of pre-peritoneal fat. LEV, lower epigastric vessels; RA, rectus abdominis.
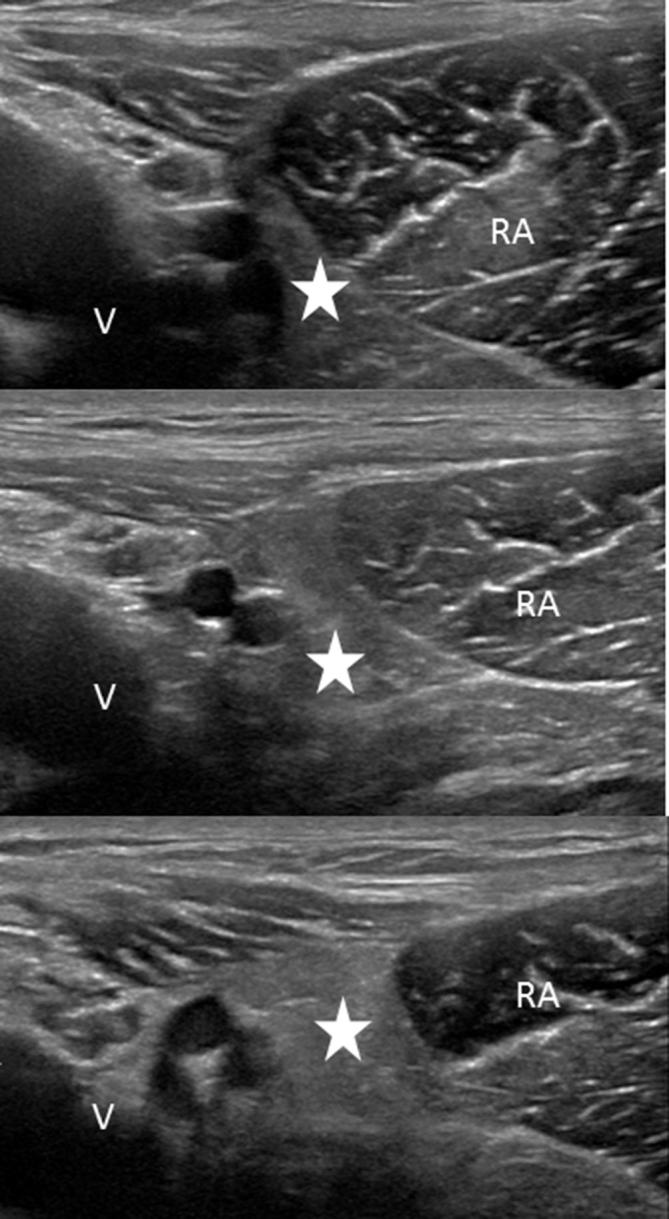
Ultrasound of a 27-year-old male soccer player with bilateral groin pain. Dynamic ultrasound at the level of Hesselbach’s triangle of the right deep inguinal ring in the transverse planes shows progressive bulging of the preperitoneal fat during Valsalva’s maneuvers (white arrow). V, vessels; RA, rectus abdominis.
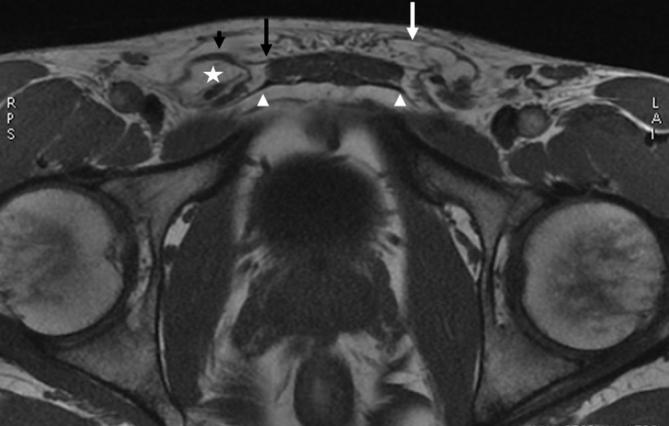
MRI of a 25-year-old male rugby player with bilateral groin pain. 3D-GE T1 weighted sequence in the axial plane shows fat within the right spermatic cord (white star), anterior wall bulging and thickening of the right external oblique aponeurosis (black arrowhead), normal distal insertion of the CT (white arrowheads) and tear of the left external oblique (white arrow). 3D, threedimensional.
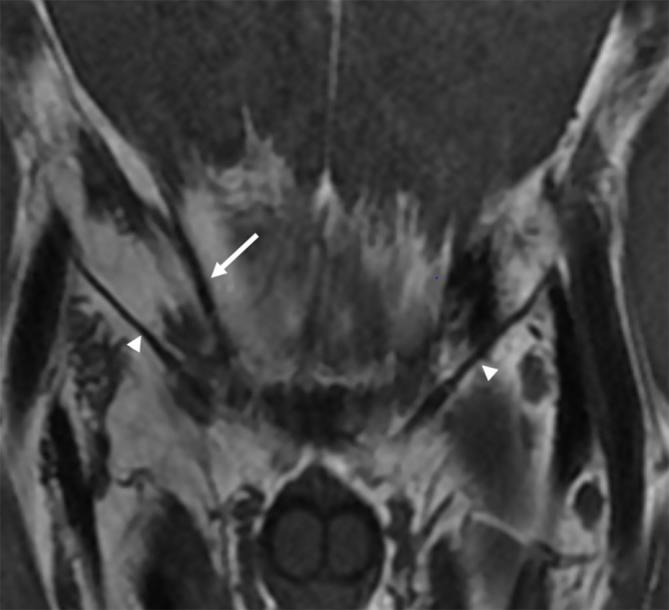
MRI of a 27-year-old male soccer player with right groin pain. 3D-GE T1 weighted sequence in the coronal plane shows thinning thickening of the inguinal ligament (arrowhead) and conjoint tendon (arrow). 3D, three-dimensional.
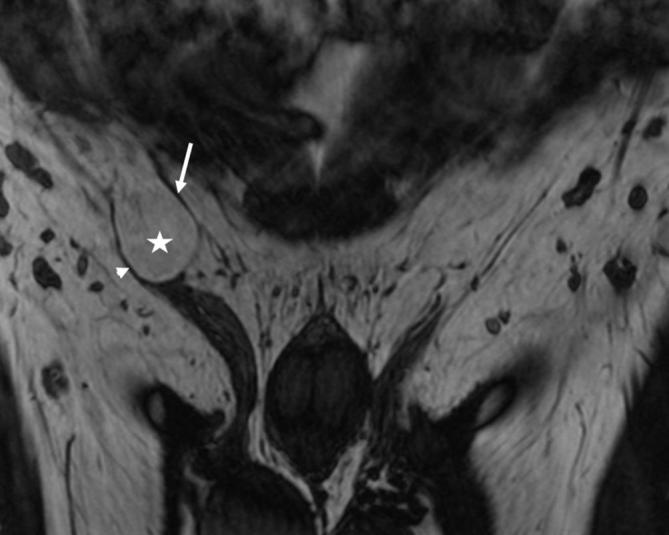
MRI of a 23-year-old male soccer player with right groin pain. 3D-GE T1 weighted sequence in the coronal plane shows fat within the right spermatic cord (white star), thinning and stretching of the inguinal ligament (arrowhead) and thinned conjoint tendon (white arrow).
Similar articles
-
Ultrasound of the athletic groin.Semin Musculoskelet Radiol. 2013 Feb;17(1):34-42. doi: 10.1055/s-0033-1333912. Epub 2013 Mar 13. Semin Musculoskelet Radiol. 2013. PMID: 23487332 Review.
-
Inguinal Hernia in Athletes: Role of Dynamic Ultrasound.Sports Health. 2017 Sep/Oct;9(5):414-421. doi: 10.1177/1941738117717009. Epub 2017 Jul 21. Sports Health. 2017. PMID: 28732177 Free PMC article.
-
Sports Hernia: Definition, Evaluation, and Treatment.JBJS Rev. 2017 Sep;5(9):e6. doi: 10.2106/JBJS.RVW.17.00022. JBJS Rev. 2017. PMID: 28937419 Review. No abstract available.
-
Imaging Athletic Groin Pain.Radiol Clin North Am. 2016 Sep;54(5):865-73. doi: 10.1016/j.rcl.2016.04.007. Radiol Clin North Am. 2016. PMID: 27545425 Review.
-
Groin pain beyond the hip: how anatomy predisposes to injury as visualized by musculoskeletal ultrasound and MRI.AJR Am J Roentgenol. 2011 Nov;197(5):1190-7. doi: 10.2214/AJR.10.4890. AJR Am J Roentgenol. 2011. PMID: 22021514 Review.
Cited by
-
Henle's Ligament: A Comprehensive Review of Its Anatomy and Terminology over Almost One and a Half Centuries.Cureus. 2018 Sep 26;10(9):e3366. doi: 10.7759/cureus.3366. Cureus. 2018. PMID: 30510876 Free PMC article. Review.
-
Optimizing Conservative Management of Groin Pain in Athletes: Insights from a Narrative Review.Life (Basel). 2025 Mar 6;15(3):411. doi: 10.3390/life15030411. Life (Basel). 2025. PMID: 40141755 Free PMC article. Review.
-
Long-standing groin pain in contact sports: a prospective case-control and MRI study.BMJ Open Sport Exerc Med. 2019 Mar 19;5(1):e000507. doi: 10.1136/bmjsem-2018-000507. eCollection 2019. BMJ Open Sport Exerc Med. 2019. PMID: 31191965 Free PMC article.
-
What the Radiologist Needs to Know About Sport Hernias: A Systematic Review of the Current Literature.Diagnostics (Basel). 2025 Mar 20;15(6):785. doi: 10.3390/diagnostics15060785. Diagnostics (Basel). 2025. PMID: 40150127 Free PMC article. Review.
-
Anatomical Features in Inguinal-Pubic-Adductor Area That May Contribute to Gender Difference in Susceptibility to Groin Pain Syndrome.J Pers Med. 2024 Aug 14;14(8):860. doi: 10.3390/jpm14080860. J Pers Med. 2024. PMID: 39202051 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
