

Examining cognition across the bipolar/schizophrenia diagnostic spectrum
- PMID: 29947606
- PMCID: PMC6019354
- DOI: 10.1503/jpn.170076
Examining cognition across the bipolar/schizophrenia diagnostic spectrum
Abstract
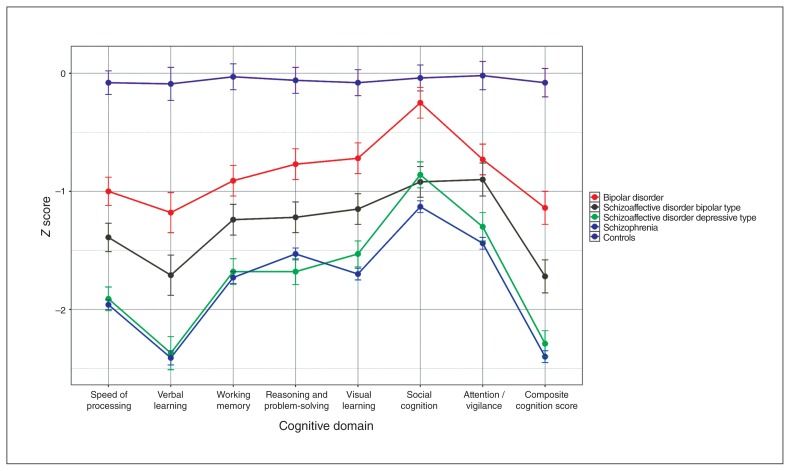
Background: Cognitive impairments are well-established features of schizophrenia, but there is ongoing debate about the nature and degree of cognitive impairment in patients with schizoaffective disorder and bipolar disorder. We hypothesized that there is a spectrum of increasing impairment from bipolar disorder to schizoaffective disorder bipolar type, to schizoaffective disorder depressive type and schizophrenia.
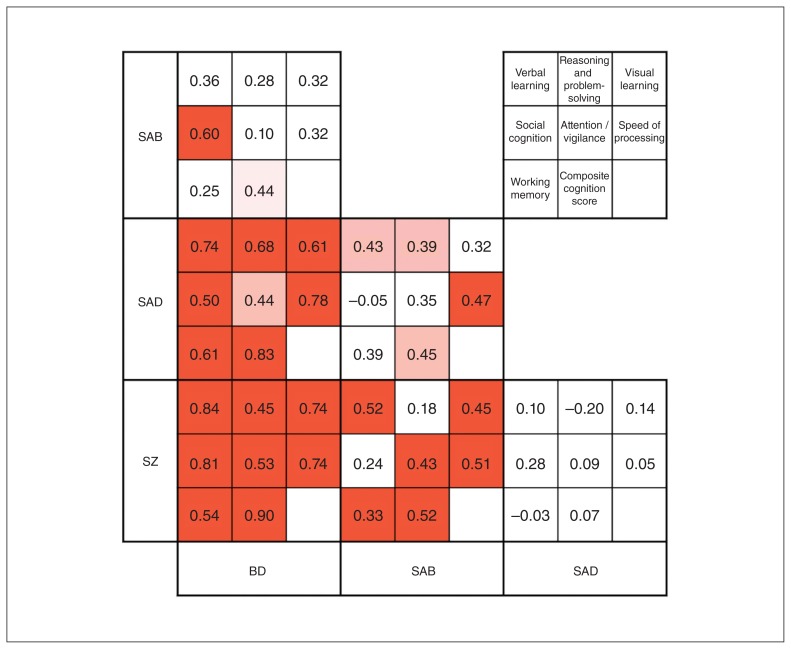
Methods: We compared performance on the Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) Consensus Cognitive Battery between participants with schizophrenia (n = 558), schizoaffective disorder depressive type (n = 112), schizoaffective disorder type (n = 76), bipolar disorder (n = 78) and healthy participants (n = 103) using analysis of covariance with post hoc comparisons. We conducted an ordinal logistic regression to examine whether cognitive impairments followed the hypothesized spectrum from bipolar disorder (least severe) to schizophrenia (most severe). In addition to categorical diagnoses, we addressed the influence of symptom domains, examining the association between cognition and mania, depression and psychosis.
Results: Cognitive impairments increased in severity from bipolar disorder to schizoaffective disorder bipolar type, to schizophrenia and schizoaffective disorder depressive type. Participants with schizophrenia and schizoaffective disorder depressive type showed equivalent performance (d = 0.07, p = 0.90). The results of the ordinal logistic regression were consistent with a spectrum of deficits from bipolar disorder to schizoaffective disorder bipolar type, to schizophrenia/schizoaffective disorder depressive type (odds ratio = 1.98, p < 0.001). In analyses of the associations between symptom dimensions and cognition, higher scores on the psychosis dimension were associated with poorer performance (B = 0.015, standard error = 0.002, p < 0.001).
Limitations: There were fewer participants with schizoaffective disorder and bipolar disorder than schizophrenia. Despite this, our analyses were robust to differences in group sizes, and we were able to detect differences between groups.
Conclusion: Cognitive impairments represent a symptom dimension that cuts across traditional diagnostic boundaries.
Conflict of interest statement
Figures
References
-
- Kasanin J. The acute schizoaffective psychoses. Am J Psychiatry. 1933;90:97–126. - PubMed
-
- Cheniaux E, Landeira-Fernandez J, Lessa Telles L, et al. Does schizoaffective disorder really exist? A systematic review of the studies that compared schizoaffective disorder with schizophrenia or mood disorders. J Affect Disord. 2008;106:209–17. - PubMed
-
- Crow TJ. Nature of the genetic contribution to psychotic illness — a continuum viewpoint. Acta Psychiatr Scand. 1990;81:401–8. - PubMed
-
- Benabarre A, Vieta E, Colom F, et al. Bipolar disorder, schizoaffective disorder and schizophrenia: epidemiologic, clinical and prognostic differences. Eur Psychiatry. 2001;16:167–72. - PubMed
