

Immunotherapy-induced pneumonitis: cases report
- PMID: 29947645
- PMCID: PMC6019244
- DOI: 10.1590/S1679-45082018RC4030
Immunotherapy-induced pneumonitis: cases report
Abstract
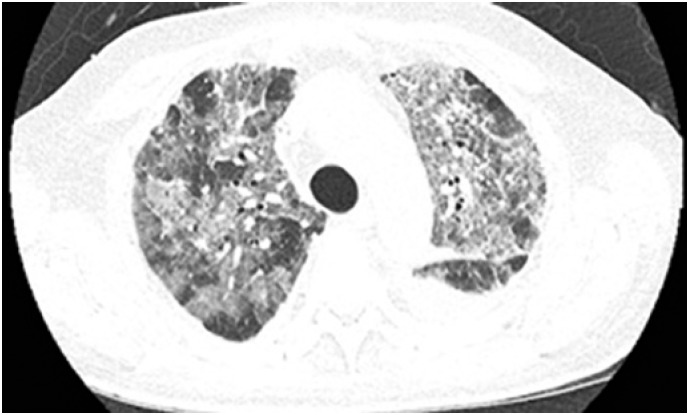
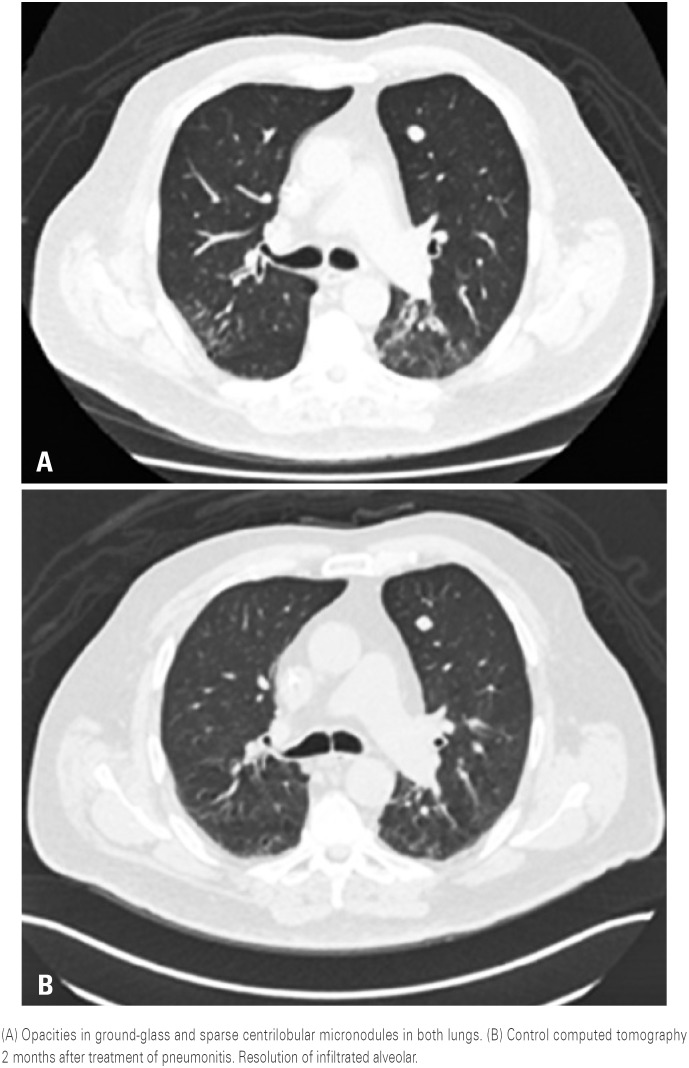
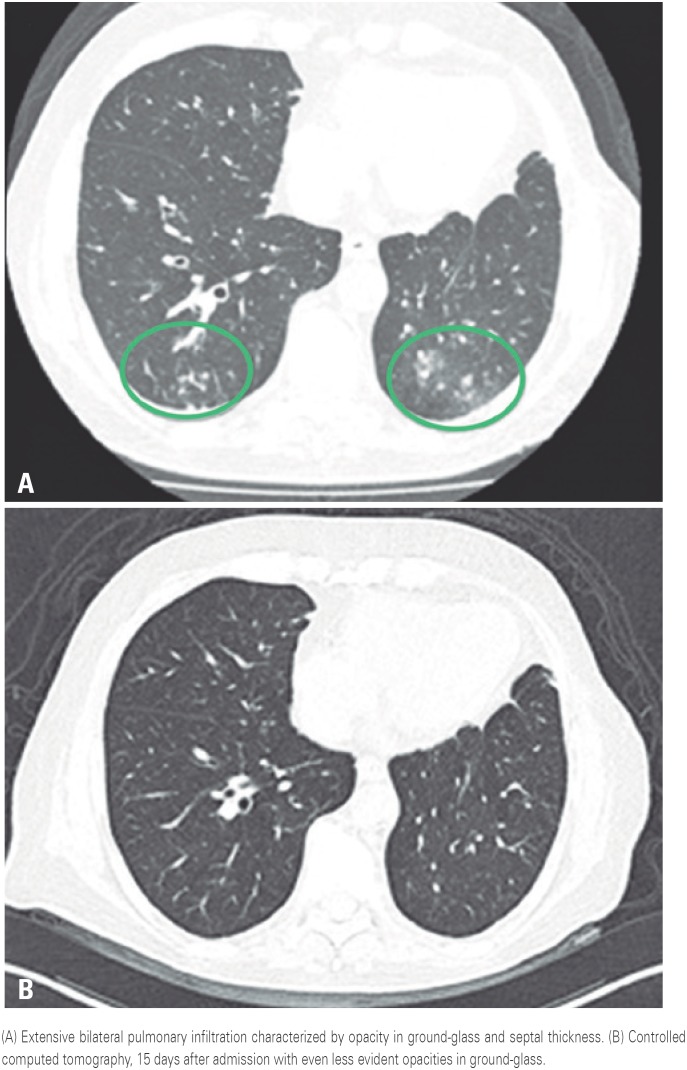
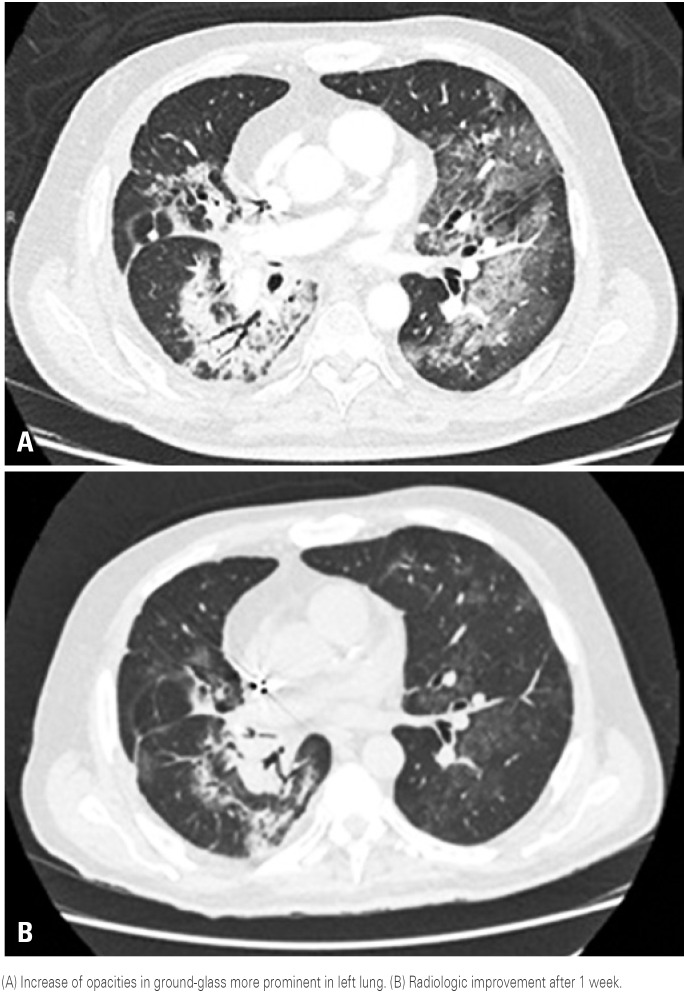
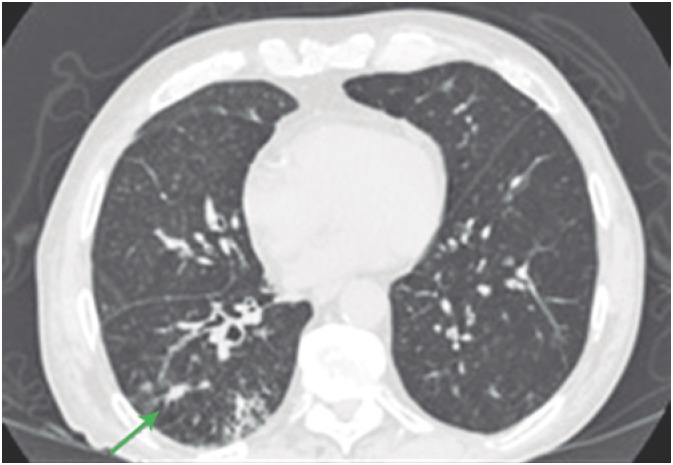
Immunotherapy-induced pneumonitis is a rare complication with incidence estimated around 3%. This disease is difficult to diagnose and has great morbidity. For this reason, it became a challenge for oncologists and emergencists. We reviewed the case of five patients who used anti-PD1 (program cell death receptor antagonist 1) for antineoplastic treatment and developed treatment-induced pneumonitis. All patients had respiratory problems because of immunotherapy and presence of ground-glass radiologic change. Among all patients, only one had grade 5 pneumonitis, and delaying to begin corticosteroid therapy and worsening in clinical picture led to patient death. Other four patients with symptomatic grade 2 pneumonitis underwent corticosteroid therapy and had improvement in clinical and radiologic picture. Two patients were treated after an episode of pneumonitis, and no new pulmonary complications were observed until the end of this study. Immunotherapy-induced pneumonitis, although uncommon, can be potentially fatal. Medical team has the responsibility to pay attention for most common symptoms of the disease such as cough and dyspnea and conduct an early diagnosis and effective early treatment with corticosteroids.
A pneumonite secundária à imunoterapia é uma complicação rara, com incidência estimada em cerca de 3%. No entanto, trata-se de uma intercorrência de difícil diagnóstico e com grande morbidade, que tem se tornado um desafio para oncologistas e emergencistas. Foram revisados os casos de cinco pacientes que fizeram uso de anti-PD1 (program cell death receptor antagonist 1) para tratamento antineoplásico e que evoluíram com quadro de pneumonite induzida pelo tratamento. Todos os pacientes apresentaram sintomas respiratórios em vigência de tratamento, com imunoterapia e presença de alteração radiológica em vidro fosco. Dentre estes pacientes, apenas um apresentou pneumonite grau 5, com atraso na introdução de corticoidoterapia, indo a óbito em decorrência do quadro. Os outros quatro pacientes apresentaram pneumonite grau 2, sintomática, sendo tratados com corticoidoterapia e evoluindo com melhora clínica e radiológica. Dois pacientes mantiveram o tratamento após o episódio de pneumonite, sem novas complicações pulmonares posteriores, até o momento. A pneumonite induzida por imunoterapia, apesar de ser um evento pouco frequente, pode acarretar grande morbidade, além de ser potencialmente fatal, cabendo à equipe médica ter atenção aos sintomas mais comuns, como tosse e dispneia, para diagnóstico precoce e tratamento efetivo, com uso precoce de corticoide.
Figures
References
-
- Nishino M, Giobbie-Hurder A, Hatabu H, Ramaiya NH, Hodi FS. Incidence of programmed cell death 1 inhibitor-related pneumonitis in patients with advanced cancer: a systematic review and meta-analysis. JAMA Oncol. 2016;2(12):1607–1616. Review. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
