

Pulsatile arterial haemodynamics in heart failure
- PMID: 29947746
- PMCID: PMC6234849
- DOI: 10.1093/eurheartj/ehy346
Pulsatile arterial haemodynamics in heart failure
Abstract
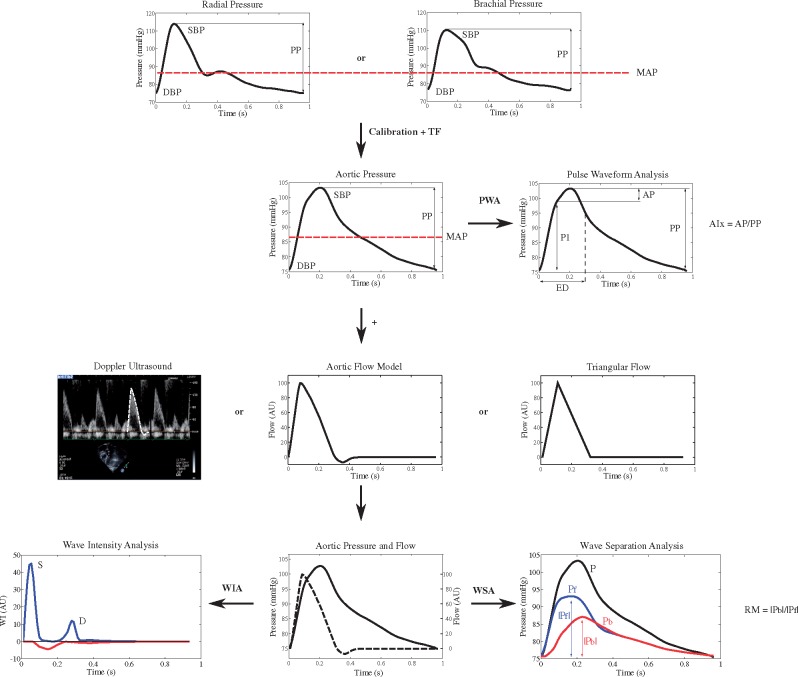
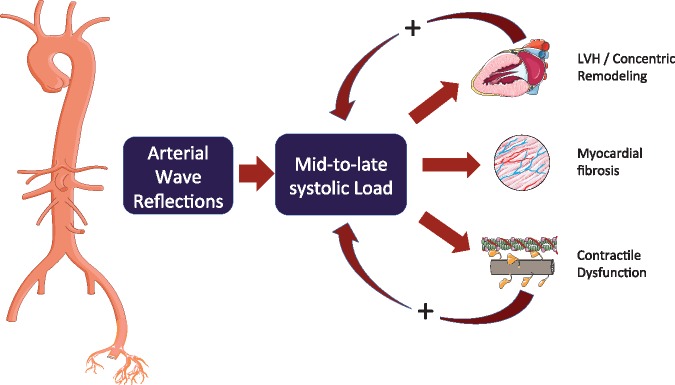
Due to the cyclic function of the human heart, pressure and flow in the circulation are pulsatile rather than continuous. Addressing pulsatile haemodynamics starts with the most convenient measurement, brachial pulse pressure, which is widely available, related to development and treatment of heart failure (HF), but often confounded in patients with established HF. The next level of analysis consists of central (rather than brachial) pressures and, more importantly, of wave reflections. The latter are closely related to left ventricular late systolic afterload, ventricular remodelling, diastolic dysfunction, exercise capacity, and, in the long-term, the risk of new-onset HF. Wave reflection may also represent a suitable therapeutic target. Treatments for HF with preserved and reduced ejection fraction, based on a reduction of wave reflection, are emerging. A full understanding of ventricular-arterial coupling, however, requires dedicated analysis of time-resolved pressure and flow signals, which can be readily accomplished with contemporary non-invasive imaging and modelling techniques. This review provides a summary of our current understanding of pulsatile haemodynamics in HF.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–2200. - PubMed
-
- Rapsomaniki E, Timmis A, George J, Pujades-Rodriguez M, Shah AD, Denaxas S, White IR, Caulfield MJ, Deanfield JE, Smeeth L, Williams B, Hingorani A, Hemingway H.. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1.25 million people. Lancet 2014;383:1899–1911. - PMC - PubMed
-
- Williamson JD, Supiano MA, Applegate WB, Berlowitz DR, Campbell RC, Chertow GM, Fine LJ, Haley WE, Hawfield AT, Ix JH, Kitzman DW, Kostis JB, Krousel-Wood MA, Launer LJ, Oparil S, Rodriguez CJ, Roumie CL, Shorr RI, Sink KM, Wadley VG, Whelton PK, Whittle J, Woolard NF, Wright JT Jr, Pajewski NM, Group SR. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged >/=75 years: a randomized clinical trial. J Am Med Assoc 2016;315:2673–2682. - PMC - PubMed
-
- Townsend RR, Wilkinson IB, Schiffrin EL, Avolio AP, Chirinos JA, Cockcroft JR, Heffernan KS, Lakatta EG, McEniery CM, Mitchell GF, Najjar SS, Nichols WW, Urbina EM, Weber T; American Heart Association Council on Hypertension. Recommendations for improving and standardizing vascular research on arterial stiffness: a scientific statement from the American Heart Association. Hypertension 2015;66:698–722. - PMC - PubMed
-
- Parragh S, Hametner B, Bachler M, Kellermair J, Eber B, Wassertheurer S, Weber T.. Determinants and covariates of central pressures and wave reflections in systolic heart failure. Int J Cardiol 2015;190:308–314. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
