

Novel approaches to restore beta cell function in prediabetes and type 2 diabetes
- PMID: 29947922
- PMCID: PMC6070408
- DOI: 10.1007/s00125-018-4658-3
Novel approaches to restore beta cell function in prediabetes and type 2 diabetes
Abstract
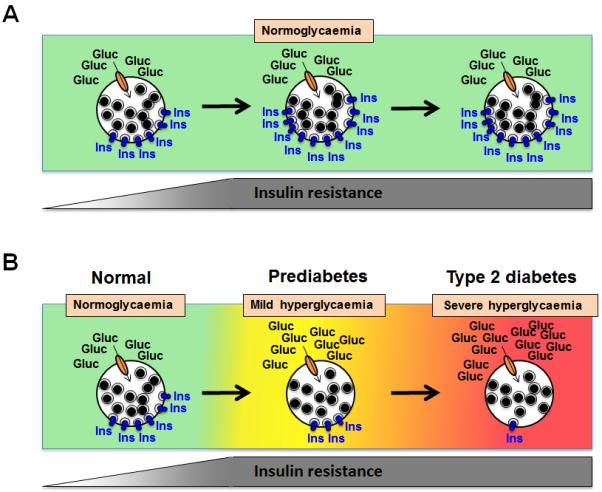
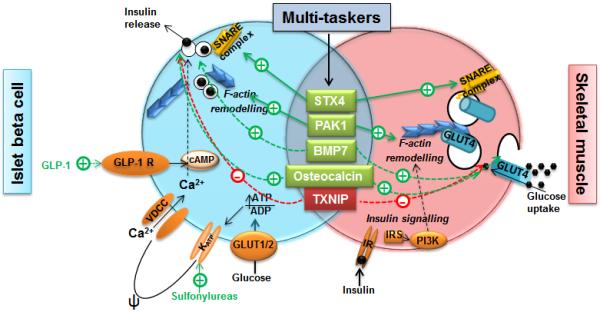
The World Health Organization estimates that diabetes prevalence has risen from 108 million in 1980 to 422 million in 2014, with type 2 diabetes accounting for more than 90% of these cases. Furthermore, the prevalence of prediabetes (impaired fasting glucose and/or impaired glucose tolerance) is more than 40% in some countries and is associated with a global rise in obesity. Therefore it is imperative that we develop new approaches to reduce the development of prediabetes and progression to type 2 diabetes. In this review, we explore the gains made over the past decade by focused efforts to improve insulin secretion by the beta cell or insulin sensitivity of target tissues. We also describe multitasking candidates, which could improve both beta cell dysfunction and peripheral insulin sensitivity. Moreover, we highlight provocative findings indicating that additional glucose regulatory tissues, such as the brain, may be key therapeutic targets. Taken together, the promise of these new multi-faceted approaches reinforces the importance of understanding and tackling type 2 diabetes pathogenesis from a multi-tissue perspective.
Keywords: Beta cell dysfunction; Insulin resistance; Insulin secretion; Obesity; Prediabetes; Review; Type 2 diabetes.
Figures
References
-
- International Diabetes Federation. [13 Nov 2017];Diabetes Atlas 8th Edition. 2017 Available from http://www.diabetesatlas.org/
-
- American Diabetes Association 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2018 Diabetes Care 2018. 41 Suppl 1 S13–S27 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
