

Outcome of Patients Treated Within and Outside a Randomized Clinical Trial on Neoadjuvant Chemoradiotherapy Plus Surgery for Esophageal Cancer: Extrapolation of a Randomized Clinical Trial (CROSS)
- PMID: 29948420
- PMCID: PMC6029046
- DOI: 10.1245/s10434-018-6554-y
Outcome of Patients Treated Within and Outside a Randomized Clinical Trial on Neoadjuvant Chemoradiotherapy Plus Surgery for Esophageal Cancer: Extrapolation of a Randomized Clinical Trial (CROSS)
Abstract
Background: Randomized clinical trials (RCTs) can provide a high level of evidence for medical decision making, but it is unclear if the results apply to patients treated outside such trials.
Objective: The aim of this study was to retrospectively compare outcomes of patients with esophageal cancer treated within and outside an RCT.
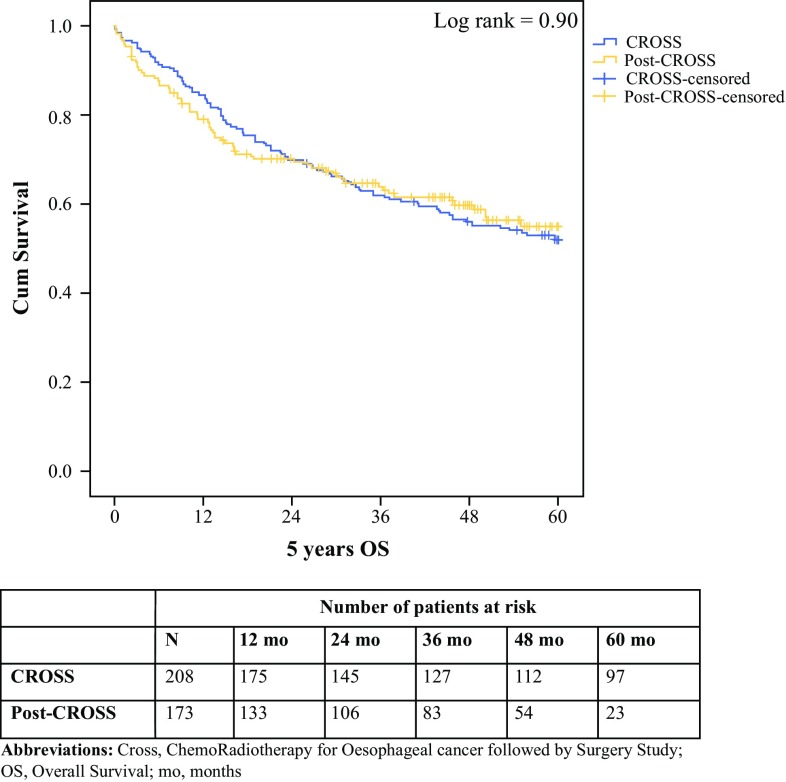
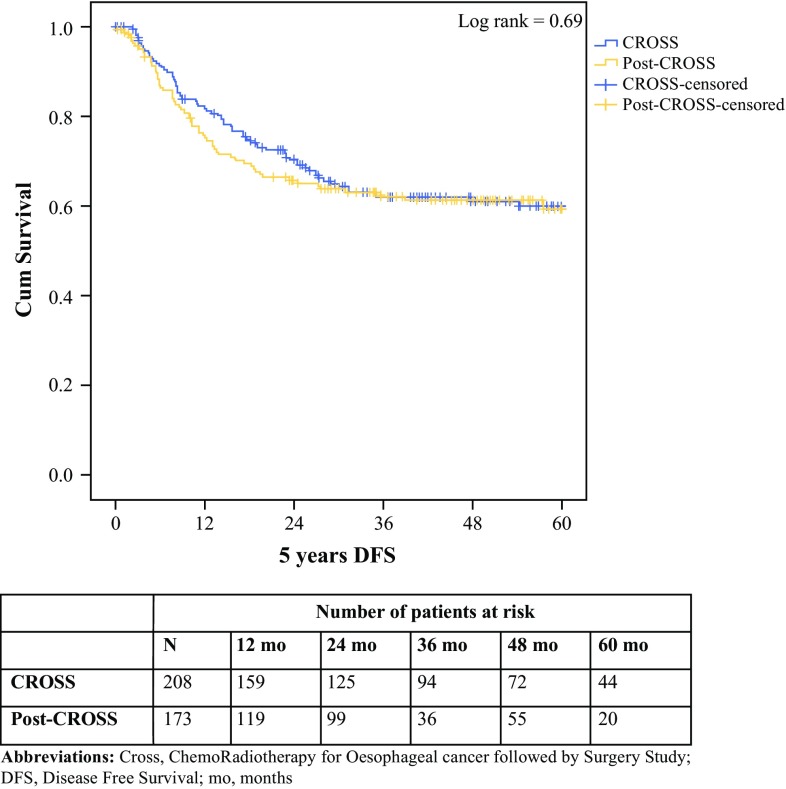
Methods: All patients receiving neoadjuvant chemoradiotherapy (nCRT) plus surgery for esophageal cancer between 2002 and 2008 (ChemoRadiotherapy for Esophageal cancer followed by Surgery Study [CROSS] cohort) who participated in multicenter, phase II-III trials were compared with patients who underwent the same treatment outside the trial between 2008 and 2013 (post-CROSS cohort). The differences between these cohorts were analyzed using t tests, while logistic regression models were used to evaluate adverse events. Overall and disease-free survival were calculated using the Kaplan-Meier method and Cox regression analyses.
Results: A total of 208 CROSS patients and 173 post-CROSS patients were included in this study. Patients from the post-CROSS cohort were older, had more co morbidities, and had poorer performance status. Clinical N stage, but not cT stage, was worse in the post-CROSS cohort. There were no statistically significant differences in adverse events (pulmonary, cardiac, or anastomotic complications) or survival between the comparison cohorts.
Conclusion: The outcomes of patients treated with nCRT plus esophagectomy for cancer have a high external consistency and can be extrapolated to the daily practice of physicians involved in the treatment and care of esophageal cancer patients.
Conflict of interest statement
There are no financial interests or potential conflicts of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
