

Transitions of Care for Postoperative Opioid Prescribing in Previously Opioid-Naïve Patients in the USA: a Retrospective Review
- PMID: 29948809
- PMCID: PMC6153216
- DOI: 10.1007/s11606-018-4463-1
Transitions of Care for Postoperative Opioid Prescribing in Previously Opioid-Naïve Patients in the USA: a Retrospective Review
Abstract
Background: New persistent opioid use is a common postoperative complication, with 6% of previously opioid-naïve patients continuing to fill opioid prescriptions 3-6 months after surgery. Despite these risks, it is unknown which specialties prescribe opioids to these vulnerable patients.
Objective: To identify specialties prescribing opioids to surgical patients who develop new persistent opioid use.
Design, setting, and participants: Using a national dataset of insurance claims, we identified opioid-naïve patients aged 18-64 years undergoing surgical procedures (2008-2014) who continued filling opioid prescriptions 3 to 6 months after surgery. We then examined opioid prescriptions claims during the 12 months after surgery, and identified prescribing physician specialty using National Provider Identifier codes.
Main measures: Percentage of opioid prescriptions provided by each specialty evaluated at 90-day intervals during the 12 months after surgery.
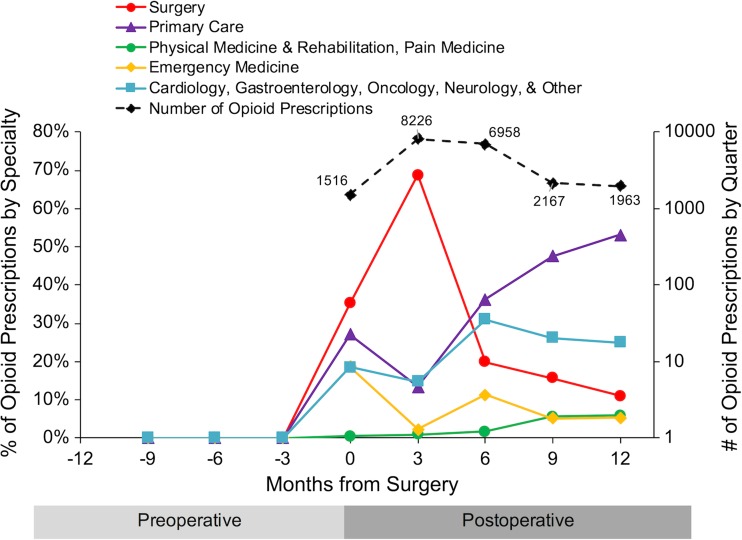
Key results: We identified 5276 opioid-naïve patients who developed new persistent opioid use. During the first 3 months after surgery, surgeons accounted for 69% of opioid prescriptions, primary care physicians accounted for 13%, Emergency Medicine accounted for 2%, Physical Medicine & Rehabilitation (PM&R)/Pain Medicine accounted for 1%, and all other specialties accounted for 15%. In contrast, 9 to 12 months after surgery, surgeons accounted for only 11% of opioid prescriptions, primary care physicians accounted for 53%, Emergency Medicine accounted for 5%, PM&R/Pain Medicine accounted for 6%, and all other specialties provided 25%.
Conclusions: Among surgical patients who developed new persistent opioid use, surgeons provide the majority of opioid prescriptions during the first 3 months after surgery. By 9 to 12 months after surgery, however, the majority of opioid prescriptions were provided by primary care physicians. Enhanced care coordination between surgeons and primary care physicians could allow earlier identification of patients at risk for new persistent opioid use to prevent misuse and dependence.
Keywords: care transitions; health services research; patient-centered outcomes research; postoperative care; surgery.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Thiels CA, Anderson SS, Ubl DS, et al. Wide variation and overprescription of opioids after elective surgery. Ann Surg. 2017. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
