

Incidence of Hospitalization for Heart Failure and Case-Fatality Among 3.25 Million People With and Without Diabetes Mellitus
- PMID: 29950404
- PMCID: PMC6287897
- DOI: 10.1161/CIRCULATIONAHA.118.034986
Incidence of Hospitalization for Heart Failure and Case-Fatality Among 3.25 Million People With and Without Diabetes Mellitus
Abstract
Background: Recent clinical trials of new glucose-lowering treatments have drawn attention to the importance of hospitalization for heart failure as a complication of diabetes mellitus. However, the epidemiology is not well described, particularly for type 1 diabetes mellitus. We examined the incidence and case-fatality of heart failure hospitalizations in the entire population aged ≥30 years resident in Scotland during 2004 to 2013.
Methods: Date and type of diabetes mellitus diagnosis were linked to heart failure hospitalizations and deaths using the national Scottish registers. Incidence rates and case-fatality were estimated in regression models (quasi-Poisson and logistic regression respectively). All estimates are adjusted for age, sex, socioeconomic status, and calendar-year.
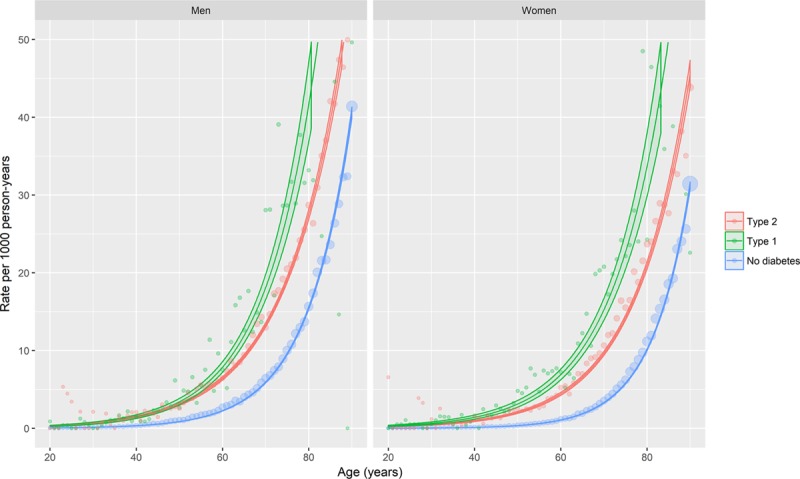
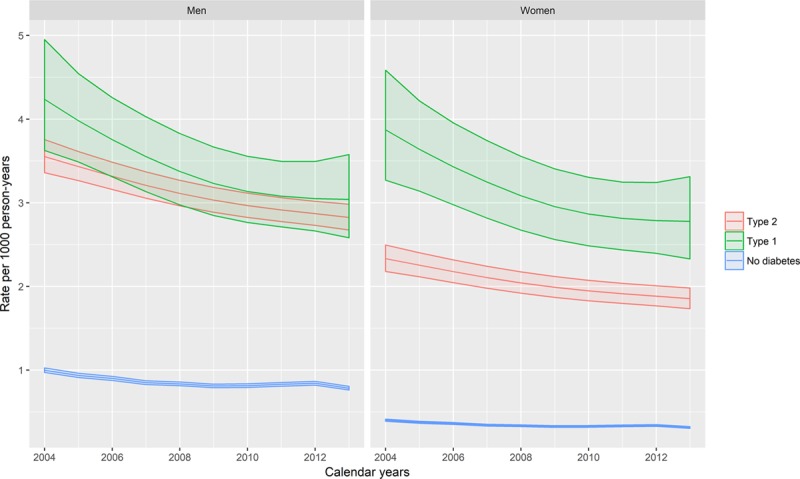
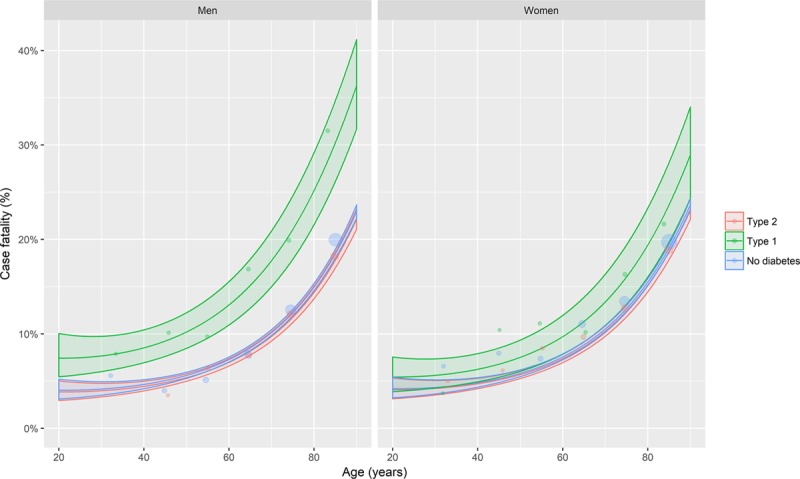
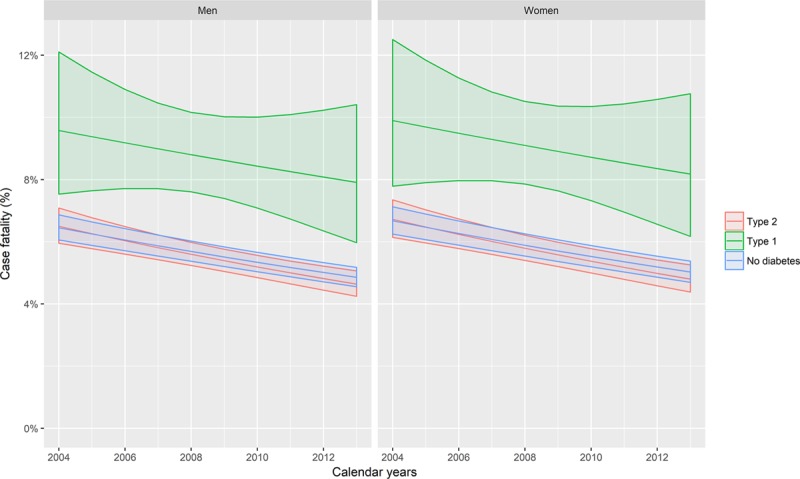
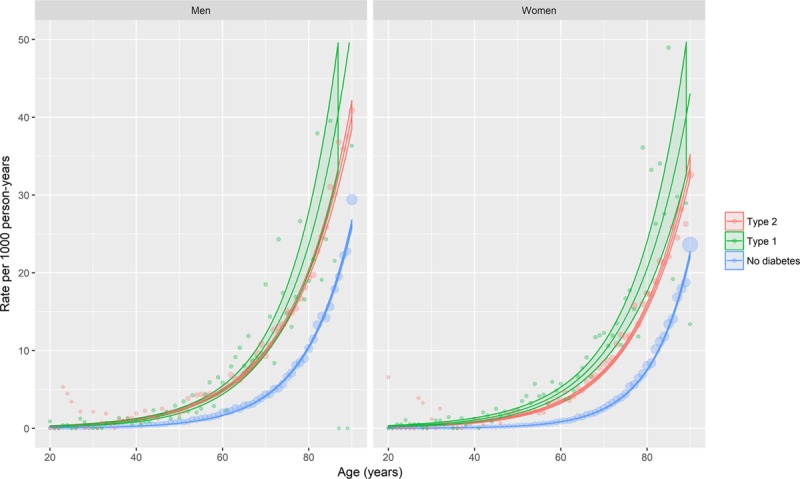
Results: Over the 10-year period of the study, among 3.25 million people there were 91, 429, 22 959, and 1313 incident heart failure events among those without diabetes mellitus, with type 2, and type 1 diabetes mellitus, respectively. The crude incidence rates of heart failure hospitalization were therefore 2.4, 12.4, and 5.6 per 1000 person-years for these 3 groups. Heart failure hospitalization incidence was higher in people with diabetes mellitus, regardless of type, than in people without. Relative differences were smallest for older men, in whom the difference was nonetheless large (men aged 80, rate ratio 1.78; 95% CI, 1.45-2.19). Rates declined similarly, by 0.2% per calendar-year, in people with type 2 diabetes mellitus and without diabetes mellitus. Rates fell faster, however, in those with type 1 diabetes mellitus (2.2% per calendar-year, rate ratio for type 1/calendar-year interaction 0.978; 95% CI, 0.959-0.998). Thirty-day case-fatality was similar among people with type 2 diabetes mellitus and without diabetes mellitus, but was higher in type 1 diabetes mellitus for men (odds ratio, 0.96; 95% CI, 0.95-0.96) and women (odds ratio, 0.98; 95% CI, 0.97-0.98). Case-fatality declined over time for all groups (3.3% per calendar-year, odds ratio per calendar-year 0.967; 95% CI, 0.961-0.973).
Conclusions: Despite falling incidence, particularly in type 1 diabetes mellitus, heart failure remains ≈2-fold higher than in people without diabetes mellitus, with higher case-fatality in those with type 1 diabetes mellitus. These findings support the view that heart failure is an under-recognized and important complication in diabetes mellitus, particularly for type 1 disease.
Keywords: diabetes mellitus; electronic health records; epidemiology; heart failure; incidence; mortality; registries.
Figures
References
-
- Cavender MA, Steg PG, Smith SC, Jr, Eagle K, Ohman EM, Goto S, Kuder J, Im K, Wilson PW, Bhatt DL REACH Registry Investigators. Impact of diabetes mellitus on hospitalization for heart failure, cardiovascular events, and death: outcomes at 4 years from the Reduction of Atherothrombosis for Continued Health (REACH) Registry. Circulation. 2015;132:923–931. doi: 10.1161/CIRCULATIONAHA.114.014796. - PubMed
-
- Rosengren A, Vestberg D, Svensson AM, Kosiborod M, Clements M, Rawshani A, Pivodic A, Gudbjörnsdottir S, Lind M. Long-term excess risk of heart failure in people with type 1 diabetes: a prospective case-control study. Lancet Diabetes Endocrinol. 2015;3:876–885. doi: 10.1016/S2213-8587(15)00292-2. - PubMed
-
- Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, Deanfield J, Smeeth L, Timmis A, Hemingway H. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1·9 million people. Lancet Diabetes Endocrinol. 2015;3:105–113. doi: 10.1016/S2213-8587(14)70219-0. - PMC - PubMed
-
- Seferović PM, Petrie MC, Filippatos GS, Anker SD, Rosano G, Bauersachs J, Paulus WJ, Komajda M, Cosentino F, de Boer RA, Farmakis D, Doehner W, Lambrinou E, Lopatin Y, Piepoli MF, Theodorakis MJ, Wiggers H, Lekakis J, Mebazaa A, Mamas MA, Tschöpe C, Hoes AW, Seferović JP, Logue J, McDonagh T, Riley JP, Milinković I, Polovina M, van Veldhuisen DJ, Lainscak M, Maggioni AP, Ruschitzka F, McMurray JJV. Type 2 diabetes mellitus and heart failure: a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2018;20:853–872. doi: 10.1002/ejhf.1170. - PubMed
-
- ISD Services | Electronic Data Research and Innovation Service (eDRIS) | Data for Research | ISD Scotland. http://www.isdscotland.org/Products-and-Services/eDRIS/Data-for-Research/. Accessed July 17, 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
