

GeriMedRisk, a telemedicine geriatric pharmacology consultation service to address adverse drug events in long-term care: a stepped-wedge cluster randomized feasibility trial protocol (ISRCTN17219647)
- PMID: 29951221
- PMCID: PMC6011190
- DOI: 10.1186/s40814-018-0300-x
GeriMedRisk, a telemedicine geriatric pharmacology consultation service to address adverse drug events in long-term care: a stepped-wedge cluster randomized feasibility trial protocol (ISRCTN17219647)
Abstract
Background: Multimorbidity, polypharmacy, and older age predispose seniors to adverse drug events (ADE). Seniors with an ADE experience greater morbidity, mortality, and health care utilization compared to their younger counterparts. To mitigate and manage ADEs among this vulnerable population, we designed a geriatric pharmacology consultation service connecting clinicians with specialist physicians and pharmacists and will investigate the feasibility and acceptability of this complex intervention in the long-term care setting, prior to conducting a larger efficacy trial.
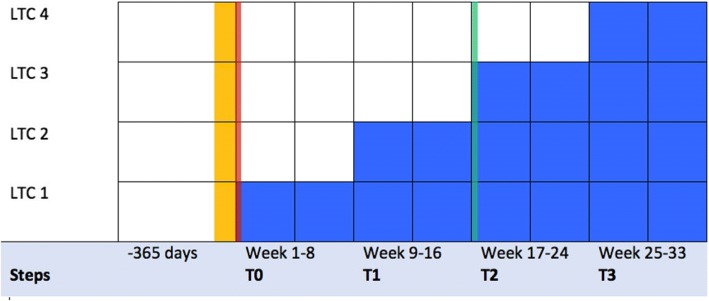
Methods/design: We will conduct a cluster randomized feasibility trial and qualitative analysis of GeriMedRisk among four long-term care homes in the Waterloo-Wellington region from May 1 to December 31, 2017. The primary outcome is the feasibility and acceptability of GeriMedRisk and the stepped-wedge cluster randomized controlled trial design. We hypothesize that GeriMedRisk is a feasible intervention and its potential to decrease falls and drug-related hospital visits can be evaluated with a stepped-wedge cluster randomized controlled trial design.
Discussion: This mixed methods study will inform a larger efficacy trial of GeriMedRisk's ability to decrease adverse drug events among seniors in the long-term care setting.
Ethics and dissemination: The Hamilton Integrated Research Ethics Board granted the approval for this study protocol 2812. We plan to disseminate the results of this study in peer-reviewed journals and also to our partners and stakeholders.
Trial registration: ISRCTN clinical trials registry, ISRCTN17219647 (March 27, 2017).
Keywords: Appropriate prescribing; Clinical trial; Cluster randomized controlled trial; Feasibility; Geriatrics; Telemedicine.
Conflict of interest statement
The Hamilton Integrated Research Ethics Board granted the approval for this study protocol 2017-2812. Following ethics approval, we will start recruiting LTC sites by proactively approaching the LTC site manager and their clinicians (February to May 2017). We will hold scheduled information sessions at each LTC site to describe the intervention and project. The study coordinator will obtain written consent from willing participants (referring clinicians). Participants may also provide verbal and written consent when they call into GeriMedRisk to request a consultation. For participating sites, we will advertise the trial through posters displayed in common clinical staff areas and directly send a flyer to patients and their caregivers which describes the option and procedure to opt out of the intervention. We will track patients who opted out (personally or by caregiver proxy) of GeriMedRisk and inform their clinician of their decision.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Canadian Institute for Health Information (CIHI) Adverse drug reaction-related hospitalizations among seniors, 2006 to 2011. 2013. p. 22.
LinkOut - more resources
Full Text Sources
Other Literature Sources
