

Cdk4/6 inhibitors and overall survival: power of first-line trials in metastatic breast cancer
- PMID: 29951582
- PMCID: PMC6018749
- DOI: 10.1038/s41523-018-0068-4
Cdk4/6 inhibitors and overall survival: power of first-line trials in metastatic breast cancer
Abstract
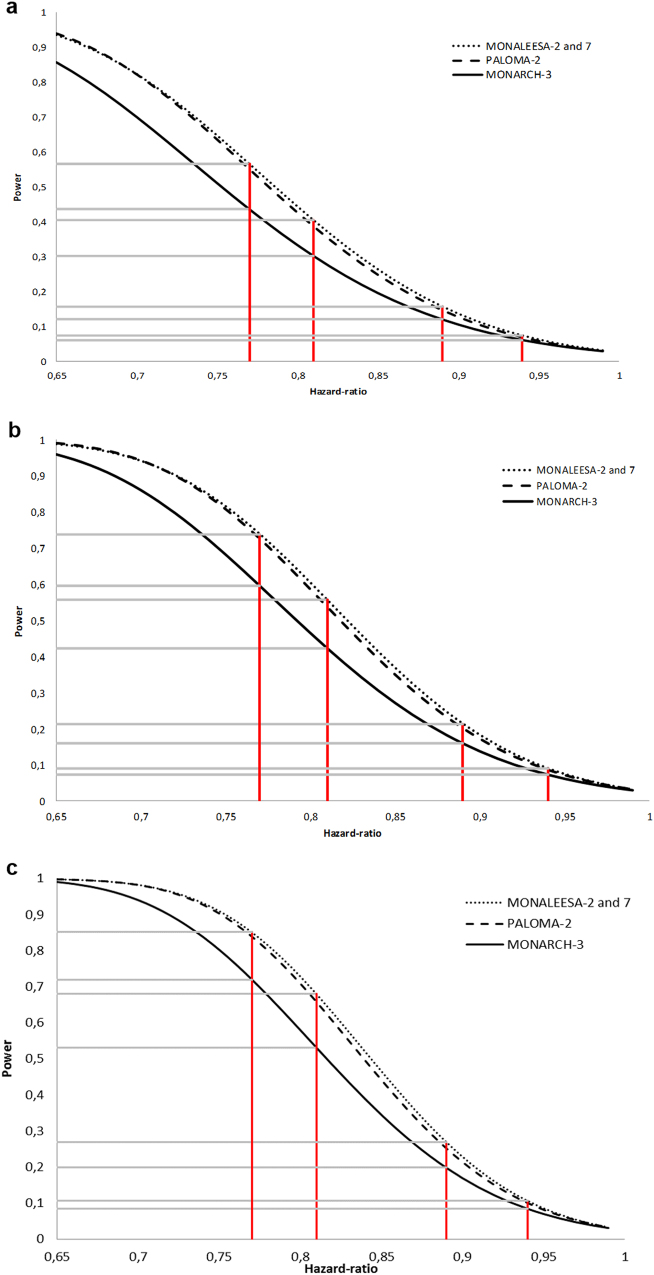
Palbociclib, ribociclib, and abemaciclib have been investigated in combination with aromatase inhibitors as first-line therapy for metastatic hormone receptor-positive breast cancer (PALOMA-2, MONALEESA-2 and MONALEESA-7, MONARCH-3 trials, respectively); pivotal trials led to absolute median progression-free survival (PFS) gain of about 15 months. We aimed to estimate, for each trial, the statistical power to demonstrate a significant gain in overall survival (OS). Power was calculated with Freedman's formula. Given the allocation ratio and the number of events, power was computed as a function of hazard ratio. We focused on four specific hazard ratio values (0.94, 0.89, 0.81, and 0.77), which are estimated to correspond to absolute 3, 6, 12, and 15 months gain in OS, respectively. For these calculations, the type I error rate was stated at 5% with a two-sided test, and we assumed that the risk of death was constant over time. PALOMA-2 and MONALEESA trials have an almost similar power despite different allocation ratios, while MONARCH-3 has a more limited power. Overall, the power of the four trials to demonstrate a statistically significant improvement in OS is less than 70% if the prolongation in median OS is ≤12 months, whatever the OS data maturity. This analysis shows that OS results are jeopardized by limited powers, and a meta-analysis might be required to demonstrate OS benefit. Conversely, if a significant OS improvement is observed in some but not at all trials, this discrepancy might be more attributable to chance than to a truly different drug efficacy.
Conflict of interest statement
F.-C. Bidard is part of advisory boards and received research grants (unrelated to this study) from Pfizer, Novartis, and Lilly. Other authors have no competing interest.
Figures
References
-
- Piccart M, et al. Everolimus plus exemestane for hormone-receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer: overall survival results from BOLERO-2†. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2014;25:2357–2362. doi: 10.1093/annonc/mdu456. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
