

Systematic review and meta-analysis of frailty as a predictor of morbidity and mortality after major abdominal surgery
- PMID: 29951615
- PMCID: PMC5989941
- DOI: 10.1002/bjs5.22
Systematic review and meta-analysis of frailty as a predictor of morbidity and mortality after major abdominal surgery
Abstract
Background: Frailty is associated with poor prognosis, but the multitude of definitions and scales of assessment makes the impact on outcomes difficult to assess. The aim of this study was to quantify the effect of frailty on postoperative morbidity and mortality, and long-term mortality after major abdominal surgery, and to evaluate the performance of different frailty metrics.
Methods: An extended literature search was performed to retrieve all original articles investigating whether frailty could affect outcomes after elective major abdominal surgery in adult populations. All possible definitions of frailty were considered. A random-effects meta-analysis was carried out for all outcomes of interest. For postoperative morbidity and mortality, overall effect sizes were estimated as odds ratios (OR), whereas the hazard ratio (HR) was calculated for long-term mortality. The potential effect of the number of domains of the frailty indices was explored through meta-regression at moderator analysis.
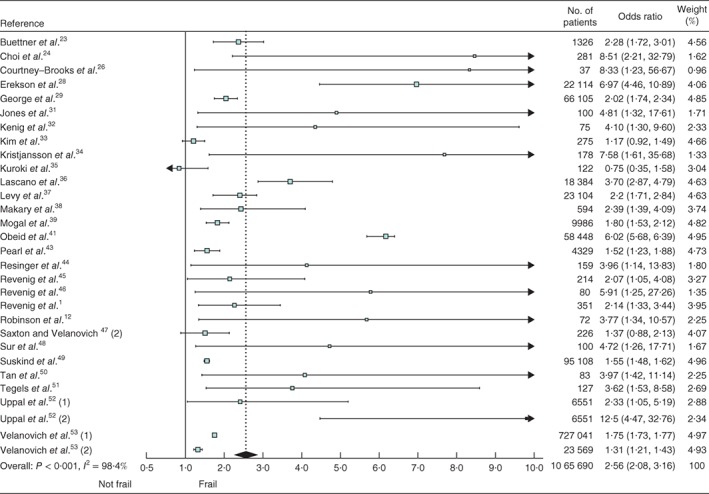
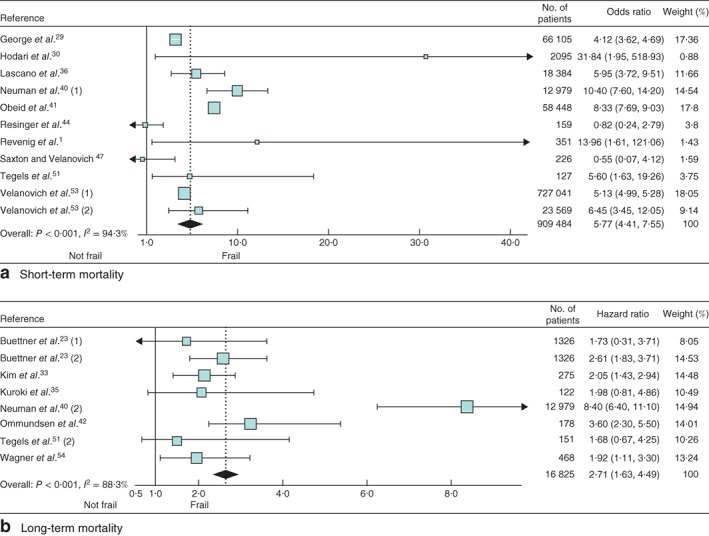
Results: A total of 35 studies with 1 153 684 patients were analysed. Frailty was associated with a significantly increased risk of postoperative major morbidity (OR 2·56, 95 per cent c.i. 2·08 to 3·16), short-term mortality (OR 5·77, 4·41 to 7·55) and long-term mortality (HR 2·71, 1·63 to 4·49). All domains were significantly associated with the occurrence of postoperative major morbidity, with ORs ranging from 1·09 (1·00 to 1·18) for co-morbidity to 2·52 (1·32 to 4·80) for sarcopenia. No moderator effect was observed according to the number of frailty components.
Conclusion: Regardless of the definition and combination of domains, frailty was significantly associated with an increased risk of postoperative morbidity and mortality after major abdominal surgery.
Figures
Comment in
-
Evidence appraisal of Sandini M, Pinotti E, Persico I, Picone D, Bellelli G, Gianotti L. Systematic review and meta-analysis of frailty as a predictor of morbidity and mortality after major abdominal surgery.BJS Open. 2017;1(5):128-137.AORN J. 2018 May;107(5):631-636. doi: 10.1002/aorn.12140. AORN J. 2018. PMID: 29708603 No abstract available.
References
-
- Revenig LM, Canter DJ, Henderson MA, Ogan K, Kooby DA, Maithel SK et al Preoperative quantification of perceptions of surgical frailty. J Surg Res 2015; 193: 583–589. - PubMed
-
- Symeonidis D, Christodoulidis G, Koukoulis G, Spyridakis M, Tepetes K. Colorectal cancer surgery in the elderly: limitations and drawbacks. Tech Coloproctol 2011; 15(Suppl 1): S47–S50. - PubMed
-
- Ferreyra G, Long Y, Ranieri VM. Respiratory complications after major surgery. Curr Opin Crit Care 2009; 15: 342–348. - PubMed
-
- Macellari F, Paciaroni M, Agnelli G, Caso V. Perioperative stroke risk in nonvascular surgery. Cerebrovasc Dis 2012; 34: 175–181. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
