

Multicentre observational study of quality of life after surgical palliation of malignant gastric outlet obstruction for gastric cancer
- PMID: 29951619
- PMCID: PMC5989952
- DOI: 10.1002/bjs5.26
Multicentre observational study of quality of life after surgical palliation of malignant gastric outlet obstruction for gastric cancer
Abstract
Background: Quality of life (QoL) is a key component in decision-making for surgical palliation, but QoL data in association with surgical palliation in advanced gastric cancer are scarce. The aim of this multicentre observational study was to examine the impact of surgical palliation on QoL in advanced gastric cancer.
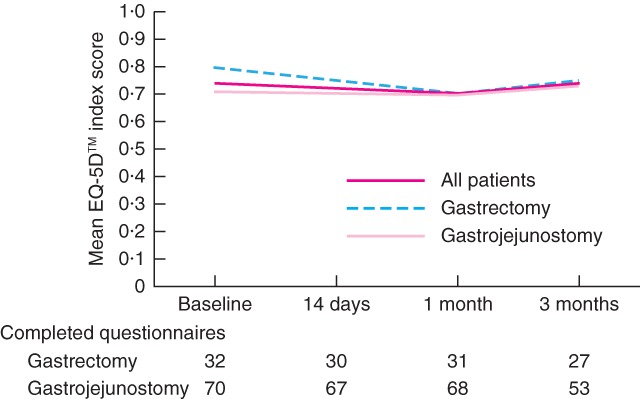
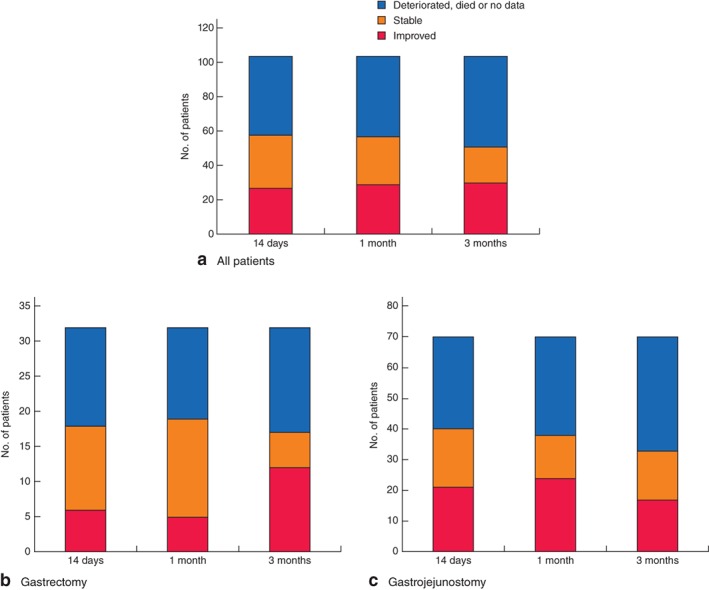
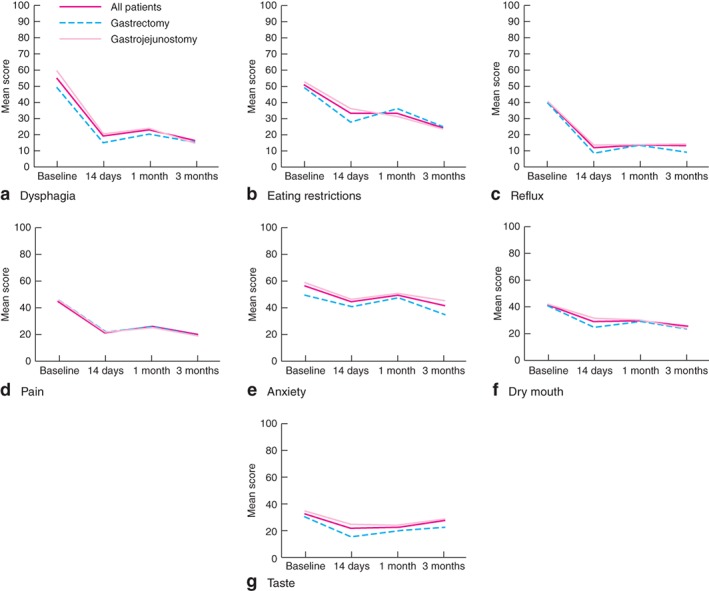
Methods: The study included patients with gastric outlet obstruction caused by incurable advanced primary gastric cancer who had no oral intake or liquid intake only. Patients underwent palliative distal/total gastrectomy or bypass surgery at the physician's discretion. The primary endpoint was change in QoL assessed at baseline, 14 days, 1 month and 3 months following surgical palliation by means of the EuroQoL Five Dimensions (EQ-5D™) questionnaire and the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire gastric cancer module (QLQ-STO22). Secondary endpoints were postoperative improvement in oral intake and surgical complications.
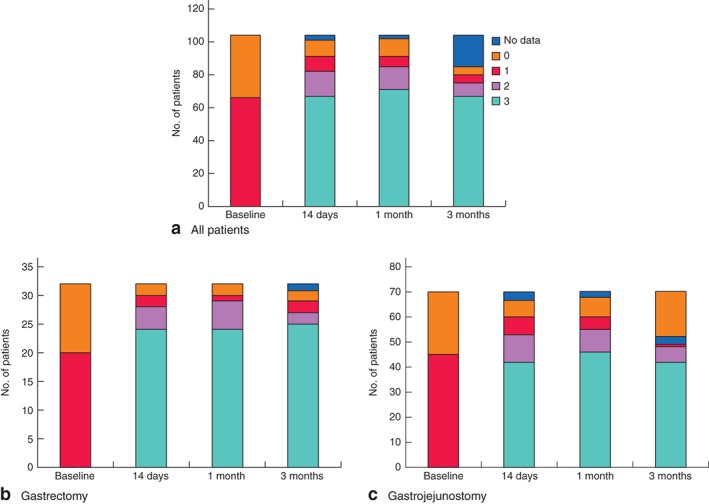
Results: Some 104 patients (23 distal gastrectomy, 9 total gastrectomy, 70 gastrojejunostomy, 2 exploratory laparotomy) were enrolled from 35 institutions. The mean EQ-5D™ utility index scores remained consistent, with a baseline score of 0·74 and the change from baseline within ± 0·05. Gastric-specific symptoms showed statistically significant improvement from baseline. The majority of patients were able to eat solid food 2 weeks after surgery and tolerated it thereafter. The rate of overall morbidity of grade III or more according to the Clavien-Dindo classification was 9·6 per cent (10 patients) and the 30-day postoperative mortality rate was 1·9 per cent (2 patients).
Conclusion: In patients with gastric outlet obstruction caused by advanced gastric cancer, surgical palliation maintained QoL while improving solid food intake, with acceptable morbidity for at least the first 3 months after surgery. Registration number 000023494 (UMIN Clinical Trials Registry).
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M et al Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015; 136: E359–E386. - PubMed
-
- Ohtsu A. Chemotherapy for metastatic gastric cancer: past, present, and future. J Gastroenterol 2008; 43: 256–264. - PubMed
-
- Gencer D, Kästle‐Larralde N, Pilz LR, Weiss A, Buchheidt D, Hochhaus A et al Presentation, treatment, and analysis of prognostic factors of terminally ill patients with gastrointestinal tumors. Onkologie 2009; 32: 380–386. - PubMed
-
- McCahill LE, Krouse R, Chu D, Juarez G, Uman GC, Ferrell B et al Indications and use of palliative surgery – results of Society of Surgical Oncology survey. Ann Surg Oncol 2002; 9: 104–112. - PubMed
-
- Velikova G, Coens C, Efficace F, Greimel E, Groenvold M, Johnson C et al Health‐related quality of life in EORTC clinical trials: 30 years of progress from methodological developments to making a real impact on oncology practice. Eur J Cancer 2012; 10: 141–149.
LinkOut - more resources
Full Text Sources
Other Literature Sources
