

Relationship between intra-abdominal hypertension, outcome and the revised Atlanta and determinant-based classifications in acute pancreatitis
- PMID: 29951620
- PMCID: PMC5989946
- DOI: 10.1002/bjs5.29
Relationship between intra-abdominal hypertension, outcome and the revised Atlanta and determinant-based classifications in acute pancreatitis
Abstract
Background: The aim of this study was to analyse the relationship between intra-abdominal hypertension (IAH) and severity of acute pancreatitis (AP) measured by the revised Atlanta classification (RAC) and determinant-based classification (DBC). Secondary objectives were to assess IAH as a predictor of morbidity and mortality in the ICU.
Methods: This prospective international observational study included patients admitted to the ICU with AP and at least one organ failure. Information was collected on demographics, severity scores at admission using RAC and DBC, organ failure, mechanical ventilation, continuous renal replacement therapy (CRRT), surgery and mortality. Maximum intra-abdominal pressure (IAP) during ICU stay was used for analysis.
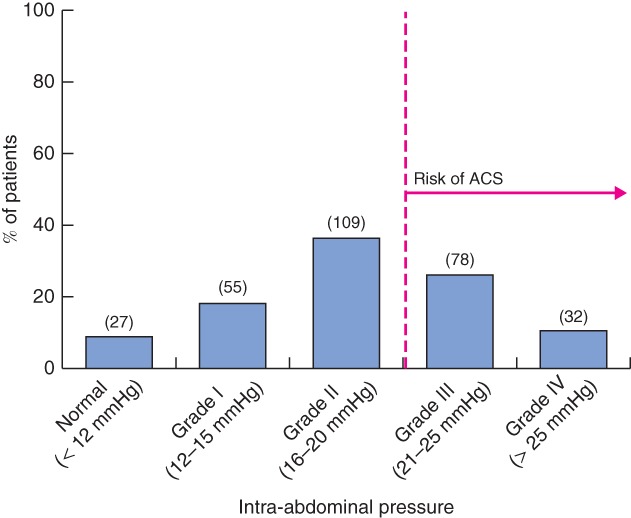
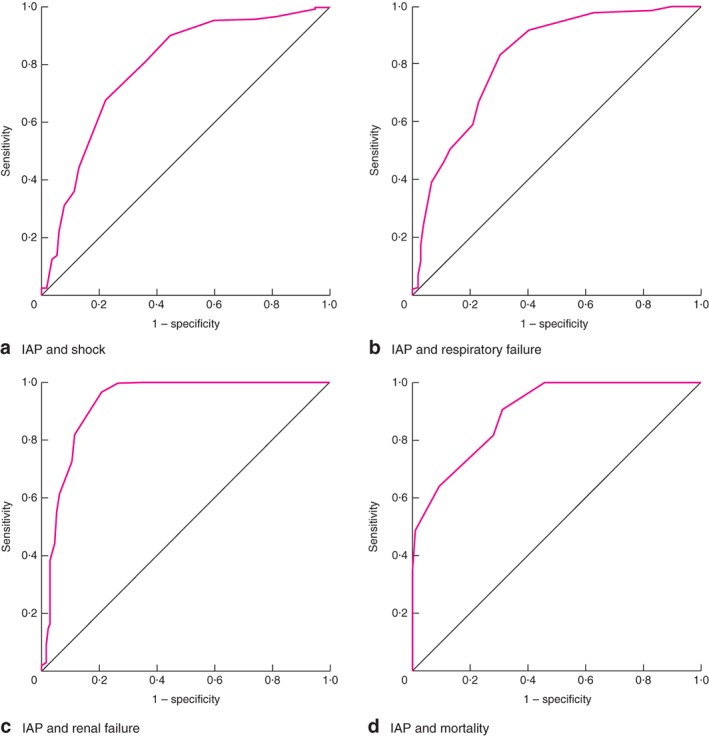
Results: Some 374 patients were included. The hospital mortality rate was 28·9 per cent. IAP was measured in 301 patients (80·5 per cent), of whom 274 (91·0 per cent) had IAH and 103 (34·2 per cent) acute compartment syndrome. A higher IAH grade was more likely in patients with severe AP (42 per cent for grade I versus 84 per cent for grade IV) and acute critical pancreatitis (9 versus 25 per cent; P = 0·001). Compared with grade I IAH, patients with grade IV had more infected necrosis (16 versus 28 per cent; P = 0·005), need for surgery (27 versus 50 per cent; P = 0·006), mechanical ventilation (53 versus 84 per cent; P = 0·007) and requirement for CRRT (22 versus 66 per cent; P < 0·001). IAH predicted shock (area under receiver operating characteristic (ROC) curve (AUC) 0·79, 95 per cent c.i. 0·73 to 0·84), respiratory failure (AUC 0·82, 0·77 to 0·87), renal failure (AUC 0·93, 0·89 to 0·96) and mortality (AUC 0·89, 0·86 to 0·93).
Conclusion: IAH was associated with severity of AP classified according to both RAC and DBC systems. IAP grade can predict outcome of AP during ICU stay.
Figures
References
-
- Kirkpatrick AW, Roberts DJ, De Waele J, Jaeschke R, Malbrain MLNG, De Keulenaer B et al; Pediatric Guidelines Sub‐Committee for the World Society of the Abdominal Compartment Syndrome. Intra‐abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med 2013; 39: 1190–1206. - PMC - PubMed
-
- Cheatham ML, Malbrain MLNG, Kirkpatrick A, Sugrue M, Parr M, De Waele J et al Results from the international conference of experts on intra‐abdominal hypertension and abdominal compartment syndrome. II. Recommendations. Intensive Care Med 2007; 33: 951–962. - PubMed
-
- Maraví Poma E, Zubia Olascoaga F, Petrov MS, Navarro Soto S, Laplaza Santos C, Morales Alava F et al Recomendaciones para el manejo en cuidados intensivos de la pancreatitis aguda. Med Intensiva 2014; 37: 163–179. - PubMed
-
- Malbrain MLNG, Chiumello D, Cesana BM, Reintam Blaser A, Starkopf J, Sugrue M et al; WAKE‐Up! Investigators. A systematic review and individual patient data meta‐analysis on intra‐abdominal hypertension in critically ill patients: the wake‐up project. World initiative on Abdominal Hypertension Epidemiology, a Unifying Project (WAKE‐Up!). Minerva Anestesiol 2014; 80: 293–306. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
