

Systematic review of the cost-effectiveness of preoperative antibiotic prophylaxis in reducing surgical-site infection
- PMID: 29951632
- PMCID: PMC5989978
- DOI: 10.1002/bjs5.45
Systematic review of the cost-effectiveness of preoperative antibiotic prophylaxis in reducing surgical-site infection
Abstract
Background: Surgical-site infections (SSIs) increase the length of hospital admission and costs. SSI prevention guidelines include preoperative antibiotic prophylaxis. This review assessed the reporting quality and cost-effectiveness of preoperative antibiotics used to prevent SSI.
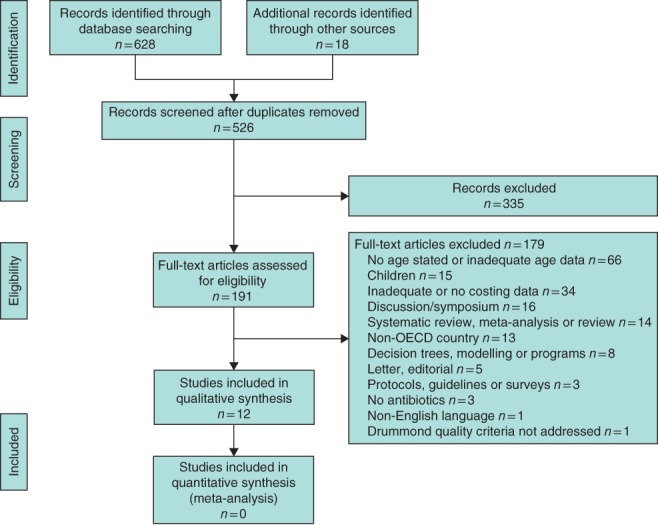
Methods: PubMed, Web of Science, Cumulative Index to Nursing and Allied Health Literature, Index of Economic Articles (EconLit), Database of Abstracts of Reviews of Effect (including the National Health Service Economic Evaluation Database) and Cochrane Central databases were searched systematically from 1970 to 2017 for articles that included costs, preoperative antibiotic prophylaxis and SSI. Included were RCTs and quasi-experimental studies conducted in Organisation for Economic Co-operation and Development countries with participants aged at least 18 years and published in English. Two reviewers assessed eligibility, with inter-rater reliability determined by Cohen's κ statistic. The Consolidated Health Economic Evaluation and Reporting Standards (CHEERS) and modified Drummond checklists were used to assess reporting and economic quality. Study outcomes and characteristics were extracted, and incremental cost-effectiveness ratios were calculated, with costs adjusted to euros (2016) (€1 = US $1·25; £1 sterling = €1·28).
Results: Twelve studies published between 1988 and 2014 were included from 646 records identified; nine were RCTs, two were nested within RCTs and one was a retrospective chart review. Study quality was highest in the nested studies. Cephalosporins (first, second and third generation) were the most frequent prophylactic interventions. Eleven studies demonstrated clinically effective interventions; ten were cost-effective (the intervention was dominant); in one the intervention was dominated by the control; and in one the intervention was more effective and more expensive than the control.
Conclusion: Preoperative antibiotic prophylaxis does reduce SSI, costs to hospitals and health providers, but the reporting of economic methods in RCTs is not standardized. Routinely nesting economic methods in RCTs would improve economic evaluations and ensure appropriate selection of prophylactic antibiotics.
Figures
References
-
- de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control 2009; 37: 387–397. - PubMed
-
- Anderson DJ. Surgical site infections. Infect Dis Clin North Am 2011; 25: 135–153. - PubMed
-
- Ozdemir S, Gulpinar K, Ozis SE, Sahli Z, Kesikli SA, Korkmaz A et al The effects of preoperative oral antibiotic use on the development of surgical site infection after elective colorectal resections: a retrospective cohort analysis in consecutively operated 90 patients. Int J Surg 2016; 33: 102–108. - PubMed
-
- Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. Infect Control Hosp Epidemiol 1992; 13: 606–608. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
