

Current Understanding of Epidemiology, Pathophysiology, and Management of Atypical Femur Fractures
- PMID: 29951870
- PMCID: PMC6061199
- DOI: 10.1007/s11914-018-0464-6
Current Understanding of Epidemiology, Pathophysiology, and Management of Atypical Femur Fractures
Abstract
Purpose of review: To summarize reports published since the 2013 American Society of Bone and Mineral Research Task Force Report on atypical femoral fractures (AFF).
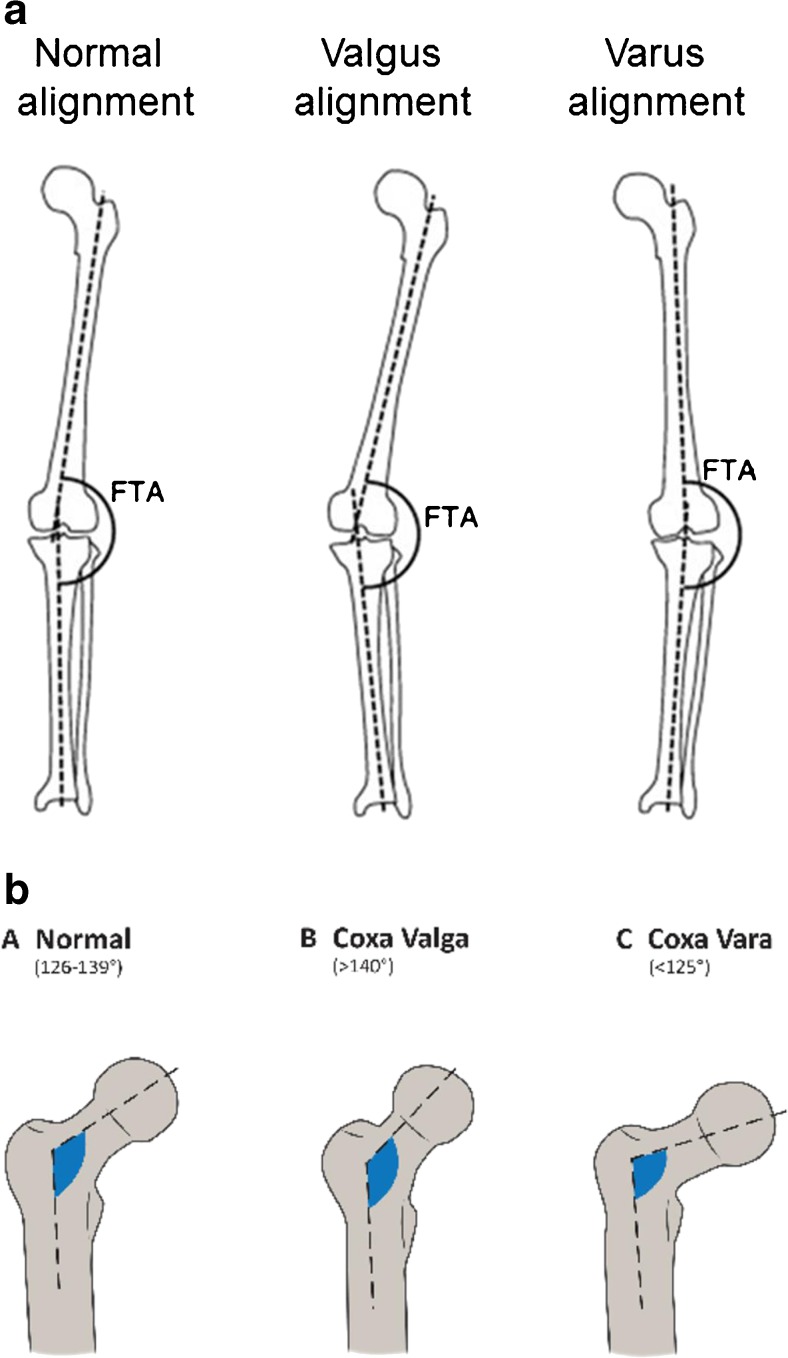
Recent findings: The absolute incidence of AFFs remains low. AFFs are primarily associated with prolonged bisphosphonate (BP) exposure, but have also been reported in unexposed patients and those receiving denosumab for osteoporosis and metastatic bone disease. Asians may be more susceptible to AFFs. Lateral femoral bowing and varus hip geometry, which increase loading forces on the lateral femoral cortex, may increase AFF risk. Altered bone material properties associated with BP therapy may predispose to AFFs by permitting initiation and increasing propagation of micro-cracks. Relevant genetic mutations have been reported in patients with AFFs. Single X-ray absorptiometry femur scans permit early detection of incomplete and/or asymptomatic AFFs. Orthopedists recommend intramedullary rods for complete AFFs and for incomplete, radiologically advanced AFFs associated with pain and/or marrow edema on MRI. Teriparatide may advance AFF healing but few data support its efficacy. Greater understanding of biological and genetic predisposition to AFF may allow characterization of individual risk prior to initiating osteoporosis therapy and help allay fear in those at low risk for this complication, which remains rare in comparison to the osteoporotic fractures prevented by antiresorptive therapy.
Keywords: Atypical femur fracture; Bisphosphonates; Bone material properties; Denosumab; Hip geometry; Teriparatide.
Conflict of interest statement
Conflict of Interest
Yu Kwang Donovan and Jessica Starr declare no conflict of interest.
Elizabeth Shane deceived grants from Amgen and Merck and is a co-chair of both ASBMR Task Forces on Atypical Femur Fractures.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures

References
-
- Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, et al. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010;25(11):2267–94. - PubMed
-
- Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2014;29(1):1–23. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
