

Clinical guidelines for primary sclerosing cholangitis 2017
- PMID: 29951926
- PMCID: PMC8930933
- DOI: 10.1007/s00535-018-1484-9
Clinical guidelines for primary sclerosing cholangitis 2017
Erratum in
-
Correction to: Clinical guidelines for primary sclerosing cholangitis 2017.J Gastroenterol. 2022 Jun;57(6):453-454. doi: 10.1007/s00535-022-01867-7. J Gastroenterol. 2022. PMID: 35294681 Free PMC article. No abstract available.
Abstract
Background: Primary sclerosing cholangitis (PSC) is relatively rare disease and pathogenesis and methods of treatments were still not established. Then, we had conducted the making clinical guidelines to manage patients with PSC based on the literature review and expert opinions. These clinical guidelines were made for the medical doctors on the management of PSC, except child case of PSC.
Methods: We had employed modified Delphi method. The production committee decided guidelines, strength of recommendations and evidence level after reviewed literatures systematically, and The Expert panel evaluated those. The Scientific Committee of the Japan Biliary Association (JBA) evaluated revised guidelines, and the Public comments were collected on web site of JBA.
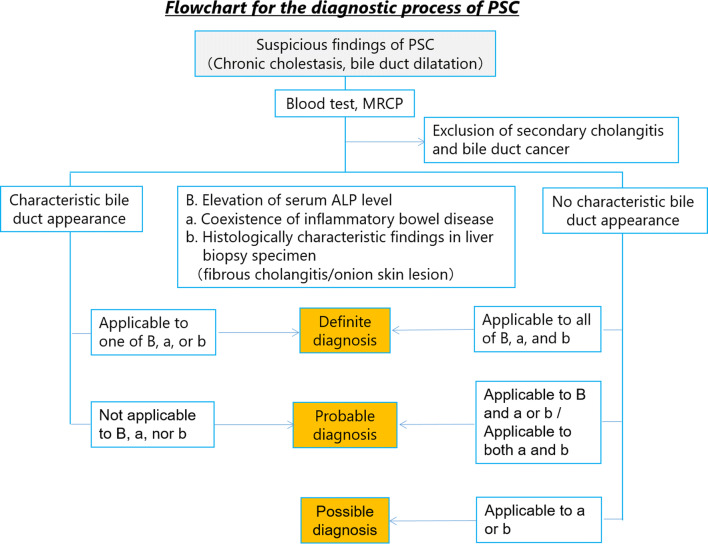
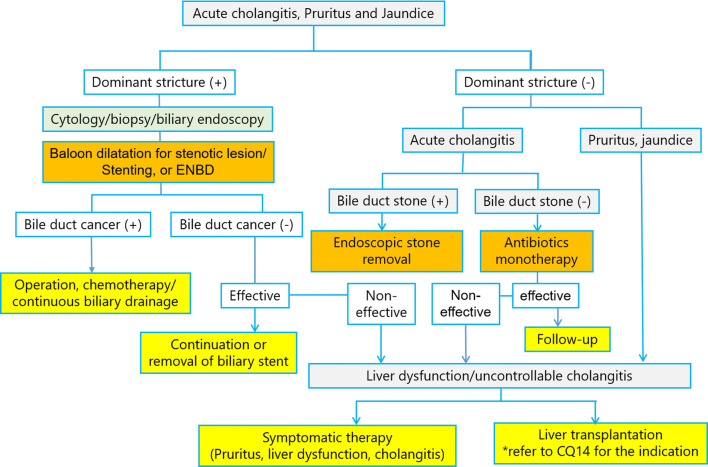
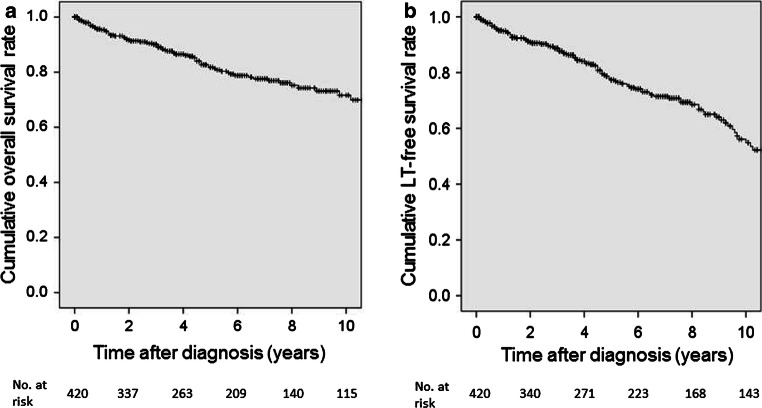
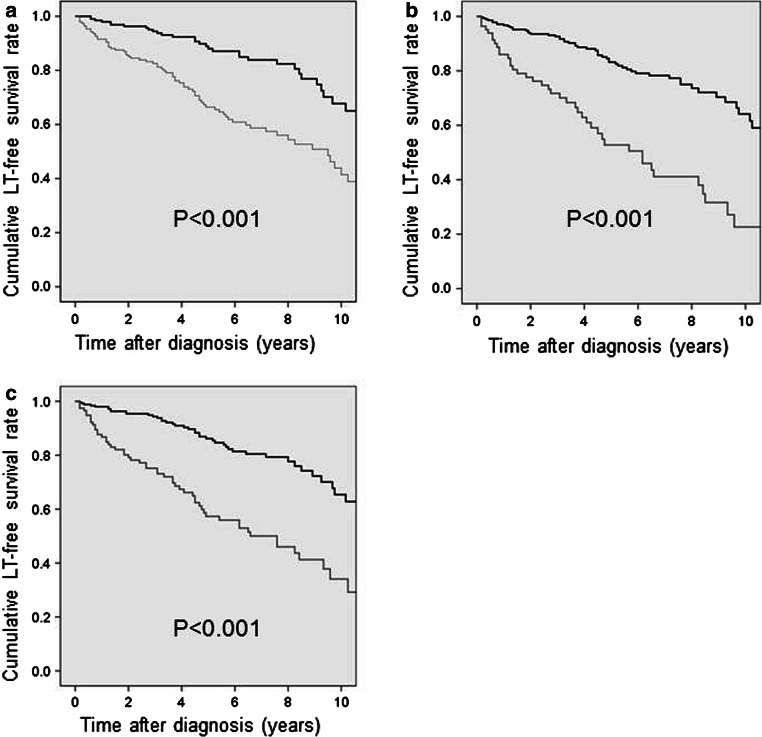
Results: We had made 16 guidelines about epidemiology/pathophysiology, diagnostics, therapy and prognosis. Also, we had made both diagnostic and therapeutic flow chart.
Conclusions: We hope that these guidelines will contribute to the improvement and development of the medical care of PSC.
Keywords: Benign biliary stricture; Cholestasis; Guidelines; Primary sclerosing cholangitis; Sclerosing cholangitis.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures

References
-
- Lindor KD, LaRusso NF. Primary sclerosing cholangitis. In: Schiff ER, editor. Disease of the liver. 9. Philadelphia: Lippincott Williams & Wilkins; 2003. pp. 673–684.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
