

Role of immune cells in hypertension
- PMID: 29952002
- PMCID: PMC6534777
- DOI: 10.1111/bph.14427
Role of immune cells in hypertension
Abstract
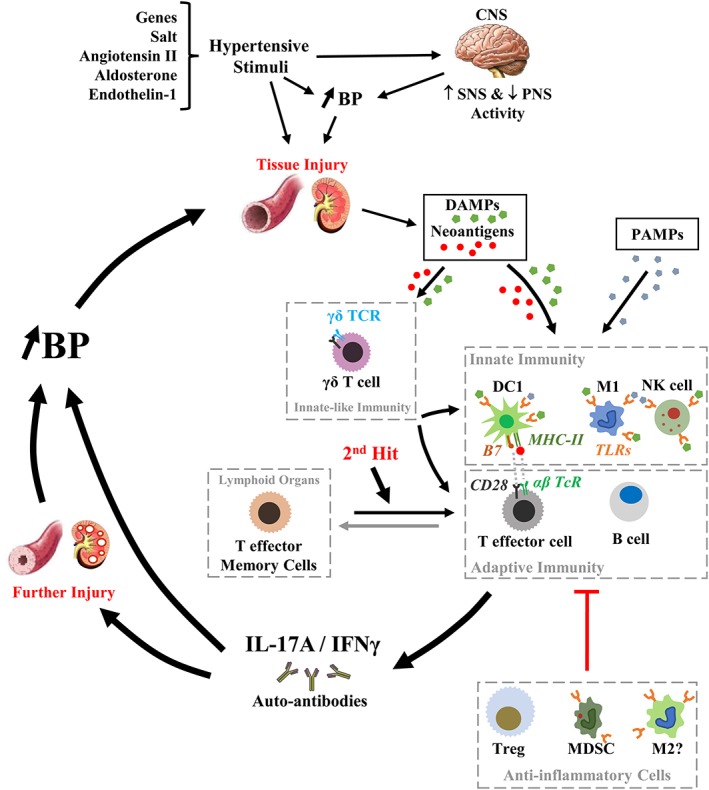
Inflammatory processes have been shown to play an important role in the mechanisms involved in the pathogenesis of hypertension. Innate and adaptive immune responses participate in BP elevation and end-organ damage. Here, we discuss recent studies focusing on novel inflammatory and immune mechanisms that play roles in BP elevation. Different subpopulations of cells involved in innate and adaptive immune responses, such as dendritic cells, monocytes/macrophages and NK cells, on the one hand, and B and T lymphocytes, on the other, contribute to the vascular and kidney injury in hypertension. Unconventional innate-like T cells such as γδ T cells also participate in hypertensive mechanisms by priming both innate and adaptive immune cells, contributing to trigger vascular inflammation and BP elevation. These cells exert their effects in part via production of various cytokines including pro-inflammatory IFN-γ and IL-17 and anti-inflammatory IL-10. The present review summarizes some of these immune mechanisms that participate in the pathophysiology of hypertension. LINKED ARTICLES: This article is part of a themed section on Immune Targets in Hypertension. To view the other articles in this section visit http://onlinelibrary.wiley.com/doi/10.1111/bph.v176.12/issuetoc.
© 2018 The British Pharmacological Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
