

Review
doi: 10.1097/GRF.0000000000000389.
Management of the Perimenopause
Affiliations
- PMID: 29952797
- PMCID: PMC6082400
- DOI: 10.1097/GRF.0000000000000389
Item in Clipboard
Review
Management of the Perimenopause
Clin Obstet Gynecol.
2018 Sep.
Abstract
Perimenopause, or the menopausal transition, represents a period of time during which newly arising symptoms can present complex management decisions for providers. Many women present to care with complaints of hot flashes, vaginal and sexual changes, altered mood and sleep, and changing bleeding patterns. The effect of these symptoms on quality of life, even before a woman enters menopause, can be significant. The appropriate evaluation and evidence-based management of women in this transition is reviewed in this article. Two case vignettes are used to highlight certain evaluation and treatment challenges.
Figures
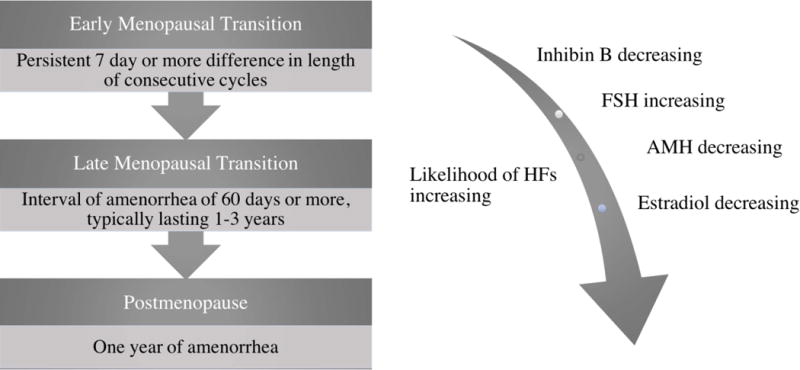
Definitions and characteristics of the Stages of Reproductive Aging, simplified from the STRAW definitions. Progression through the perimenopause is marked by increasing menstrual cycle variability that serves to define these stages. As will be discussed, this correlates with trends in hormonal levels. In addition to bleeding pattern changes, symptoms are also significant for increasingly prevalent VMS. These typically begin either during the menopausal transition or early in the postmenopausal stage.
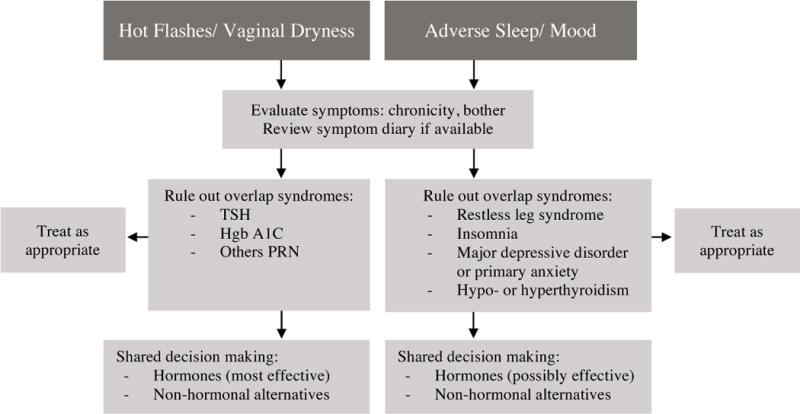
Approach to evaluation and management of menopausal symptoms. Symptoms are grouped into two main categories, from among the 4 symptom sets that are most likely related to the menopausal transition. Few symptoms mimic VMS, but because of their prevalence, ruling out thyroid disease and type 2 diabetes is prudent. Vaginal dryness can sometimes be due to conditions other than menopause (e.g. lichen sclerosus et atrophicus), and a physical examination is recommended. Restless leg syndrome and chronic insomnia often overlap with menopause-related sleep concerns, and treatment will be most effective if both problems are addressed. Primary mood disorders that are long-standing and/or severe are less likely to respond to hormone therapy (HT) alone; a thorough history will help the clinician determine whether single-agent therapy with hormones is indicated, or if co-management with a mental health professional may be more effective. Hormones are likely the most efficient path to symptom control for women with VMS or vaginal dryness; in the latter case, topical hormones may be sufficient. Women with mood and sleep issues may benefit from a trial of hormones; if not sufficiently improved, additional, non-hormonal options or co-management should be considered.
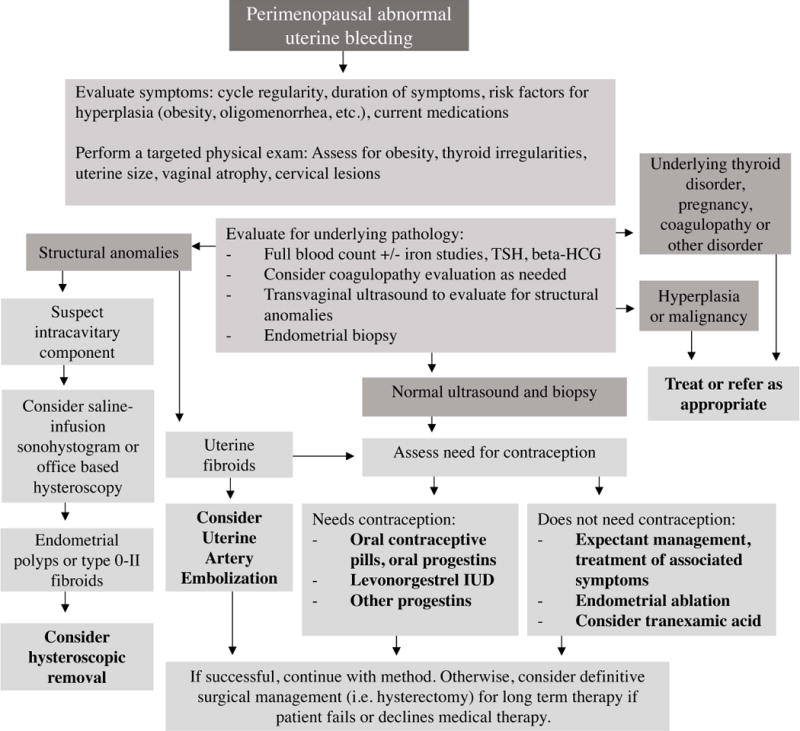
Approach to management of abnormal uterine bleeding in perimenopausal patients, taking into account appropriate evaluation, need for contraception, and management options available. As shown, management should be targeted toward underlying pathology when encountered. Otherwise, decisions should incorporate a patient-centered approach after discussion of the patient’s goals. It is important to note that, when workup has ruled out pathology necessitating medical intervention, reassurance can be provided to the patient and it is reasonable to pursue expectant management. Additionally, bleeding abnormalities may be multifactorial; anovulatory bleeding concurrent with structural abnormalities is less likely to resolve after addressing the structural component alone. When symptoms are bothersome to the patient, treatment can range from medical to surgical management, and definitive surgical management (i.e. a hysterectomy) can be considered for patients who have failed or decline other methods.
References
-
- Guthrie JR, Dennerstein L, Taffe JR, Donnelly V. Health care-seeking for menopausal problems. Climacteric. 2003;6:112–7. - PubMed
-
- Wallace RB, Sherman BM, Bean JA, Treloar AE, Schlabaugh L. Probability of menopause with increasing duration of amenorrhea in middle-aged women. Am J Obstet Gynecol. 1979;135:1021–4. - PubMed
-
- Grady D. Clinical practice. Management of menopausal symptoms. N Engl J Med. 2006;355:2338–47. - PubMed
-
- Soules MR, Sherman S, Parrott E, et al. Stages of Reproductive Aging Workshop (STRAW) J Womens Health Gend Based Med. 2001;10:843–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
