

Discrimination of pyogenic spondylitis from brucellar spondylitis on MRI
- PMID: 29952971
- PMCID: PMC6039692
- DOI: 10.1097/MD.0000000000011195
Discrimination of pyogenic spondylitis from brucellar spondylitis on MRI
Abstract
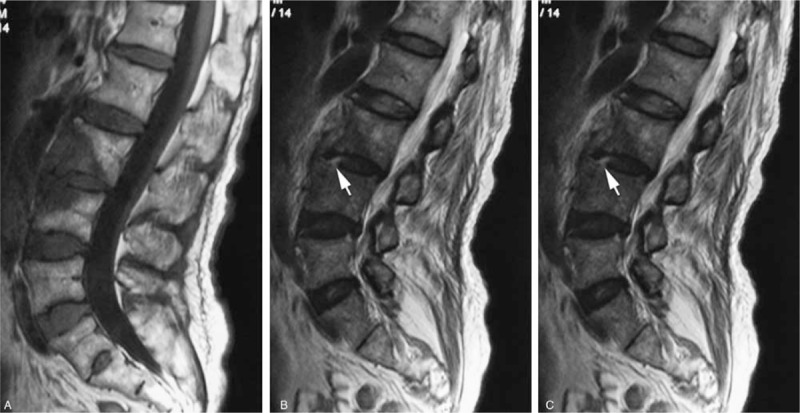
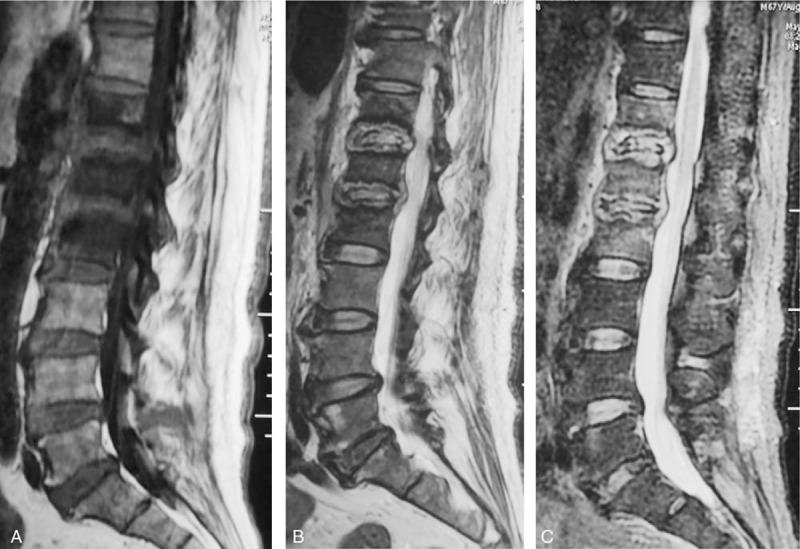
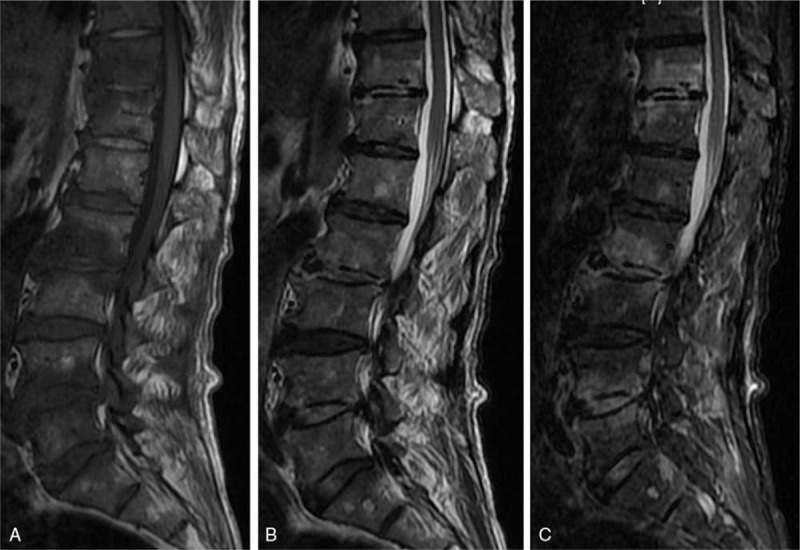
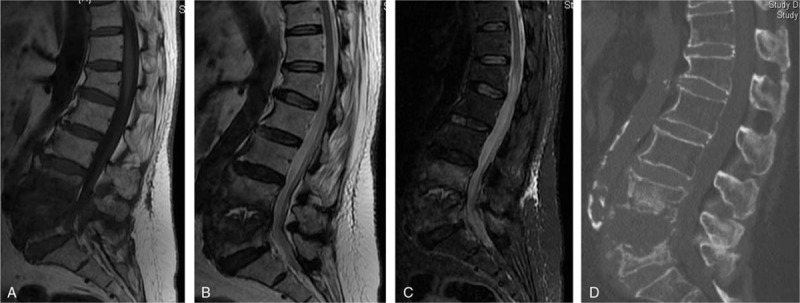
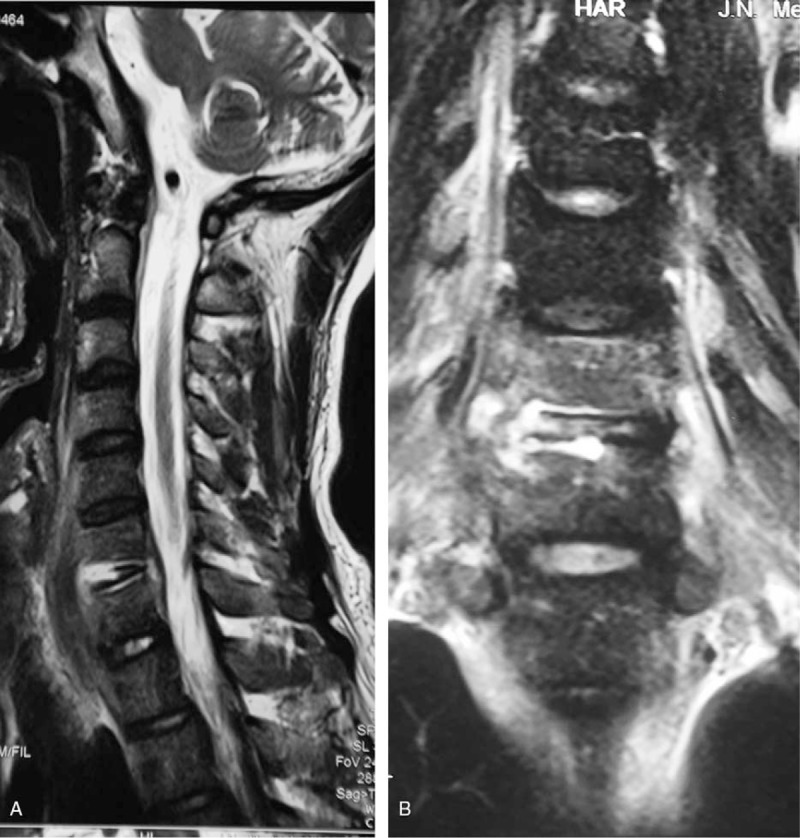
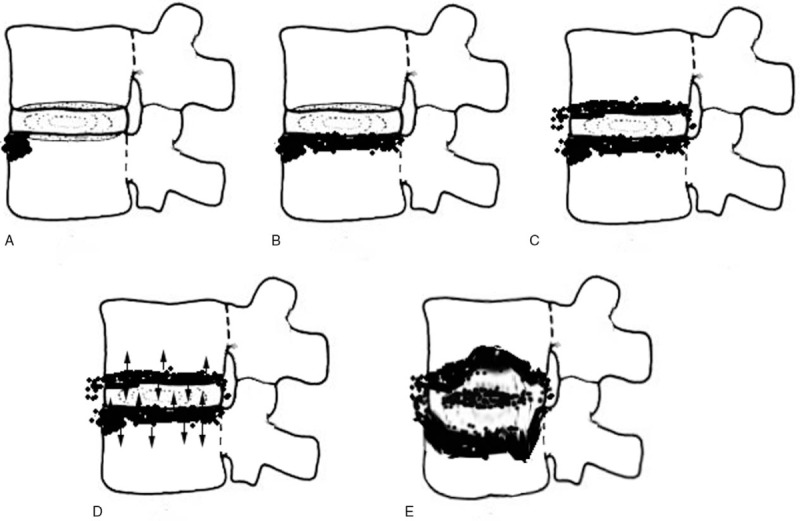
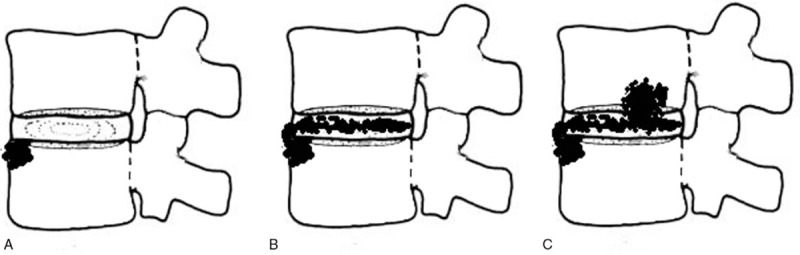
Retrospective Cross-Sectional Study.The purpose of this study was to investigate the accuracy of magnetic resonance imaging (MRI) for distinguishing between pyogenic spondylitis and brucellar spondylitis.Although pyogenic spondylodiscitis (PS) and brucellar spondylitis (BS) are common causes of spinal infections, the variety of their clinical manifestations complicates differential diagnosis. MRI may be helpful in differential diagnosis and treatment.MRI images of 64 patients who underwent MRI of the spine and with confirmed spondylitis were retrospectively reviewed. After referring to the related medical literature, we compared 32 patients with pyogenic spondylitis and 32 patients with brucellar spondylitis regarding MRI findings. Statistical analysis was performed with the chi-square test. Statistical significance was defined as P < .05.The significant differences between PS and BS on MRI findings are listed as follows (P < .05): diffuse, partial and fan-shaped hyperintense signals on middle sagittal fat-suppressed weighted images (PS: 51, 11, 3/65 vs BS:35, 18, 19/72); focal endplate destruction (PS: 9/43 vs BS:27/35); extensive end plate destruction (PS: 29/43 vs BS:8/35); ballooning change of the intravertebral space (PS: 7/32 vs BS:0/32); an inflammatory reaction line from the end plate (PS: 30/65 vs BS: 1/72); a disc invasion sign (PS: 1/28 vs BS:12/33); an inflammatory reaction line in the disc (PS: 5/28 vs BS:25/33); and 8) severe intravertebral space destruction (PS: 17/28 vs BS:12/33);MRI imaging provides useful information for the differentiation between pyogenic spondylitis and brucellar spondylitis.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Baleriaux DL, Neugroschl C. Spinal and spinal cord infection. Eur Radiol 2004;14(suppl 3):E72–83. - PubMed
-
- Tali ET. Spinal infections. Eur J Radiol 2004;50:120–33. - PubMed
-
- Mukherji SK. Spinal infections. Neuroimaging Clin N Am 2015;25:xiii. - PubMed
-
- Gold M. Magnetic resonance imaging of spinal emergencies. Top Magn Reson Imaging 2015;24:325–30. - PubMed
-
- Tali ET, Koc AM, Oner AY. Spinal brucellosis. Neuroimag Clin N Am 2015;25:233–45. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
