

The costs and cost effectiveness of providing second-trimester medical and surgical safe abortion services in Western Cape Province, South Africa
- PMID: 29953434
- PMCID: PMC6023192
- DOI: 10.1371/journal.pone.0197485
The costs and cost effectiveness of providing second-trimester medical and surgical safe abortion services in Western Cape Province, South Africa
Abstract
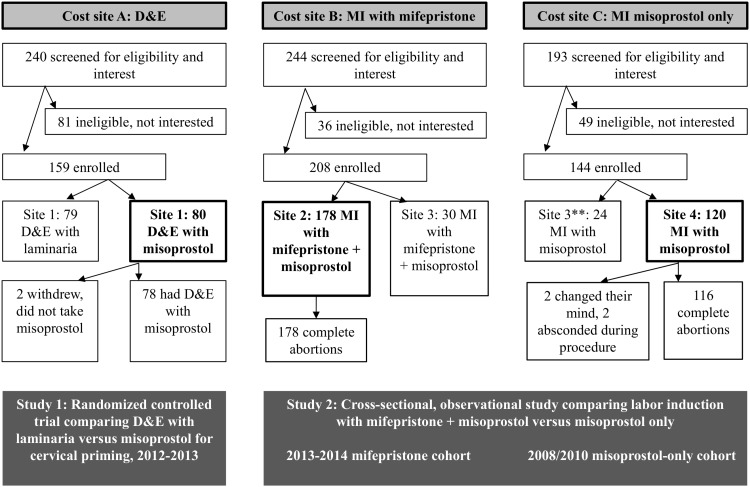
Background: In South Africa, access to second-trimester abortion services, which are generally performed using medical induction with misoprostol alone, is challenging for many women. We aimed to estimate the costs and cost effectiveness of providing three safe second-trimester abortion services (dilation and evacuation (D&E)), medical induction with mifepristone and misoprostol (MI-combined), or medical induction with misoprostol alone (MI-misoprostol)) in Western Cape Province, South Africa to aid policymakers with planning for service provision in South Africa and similar settings.
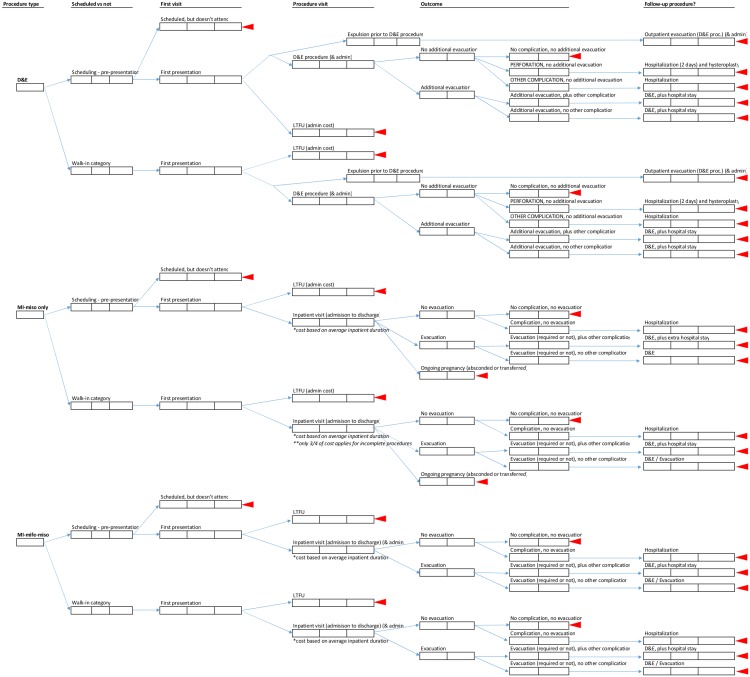
Methods: We derived clinical outcomes data for this economic evaluation from two previously conducted clinical studies. In 2013-2014, we collected cost data from three public hospitals where the studies took place. We collected cost data from the health service perspective through micro-costing activities, including discussions with site staff. We used decision tree analysis to estimate average costs per patient interaction (e.g. first visit, procedure visit, etc.), the total average cost per procedure, and cost-effectiveness in terms of the cost per complete abortion. We discounted equipment costs at 3%, and present the results in 2015 US dollars.
Results: D&E services were the least costly and the most cost-effective at $91.17 per complete abortion. MI-combined was also less costly and more cost-effective (at $298.03 per complete abortion) than MI-misoprostol (at $375.31 per complete abortion), in part due to a shortened inpatient stay. However, an overlap in the plausible cost ranges for the two medical procedures suggests that the two may have equivalent costs in some circumstances.
Conclusion: D&E was most cost-effective in this analysis. However, due to resistance from health care providers and other barriers, these services are not widely available and scale-up is challenging. Given South Africa's reliance on medical induction, switching to the combined regimen could result in greater access to second-trimester services due to shorter inpatient stays without increasing costs.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The costs and cost effectiveness of providing first-trimester, medical and surgical safe abortion services in KwaZulu-Natal Province, South Africa.PLoS One. 2017 Apr 3;12(4):e0174615. doi: 10.1371/journal.pone.0174615. eCollection 2017. PLoS One. 2017. PMID: 28369061 Free PMC article.
-
Clinical Outcomes and Women's Experiences before and after the Introduction of Mifepristone into Second-Trimester Medical Abortion Services in South Africa.PLoS One. 2016 Sep 1;11(9):e0161843. doi: 10.1371/journal.pone.0161843. eCollection 2016. PLoS One. 2016. PMID: 27583448 Free PMC article.
-
Doing more for less: identifying opportunities to expand public sector access to safe abortion in South Africa through budget impact analysis.Contraception. 2018 Feb;97(2):167-176. doi: 10.1016/j.contraception.2017.07.165. Epub 2017 Aug 3. Contraception. 2018. PMID: 28780240
-
Second trimester medical abortion with mifepristone-misoprostol and misoprostol alone: a review of methods and management.Reprod Health Matters. 2008 May;16(31 Suppl):162-72. doi: 10.1016/S0968-8080(08)31371-8. Reprod Health Matters. 2008. PMID: 18772097 Review.
-
Update on second-trimester surgical abortion.Curr Opin Obstet Gynecol. 2016 Dec;28(6):510-516. doi: 10.1097/GCO.0000000000000318. Curr Opin Obstet Gynecol. 2016. PMID: 27684047 Review.
Cited by
-
Magnitude of late presentation for induced abortion care services and the associated factors among reproductive-age women at selected hospitals in the South Gondar district of Northwest Ethiopia in 2023: a multicentred, cross-sectional study.BMJ Open. 2024 Nov 20;14(11):e081946. doi: 10.1136/bmjopen-2023-081946. BMJ Open. 2024. PMID: 39572098 Free PMC article.
-
Dilation and evacuation versus medication abortion at 15-24 weeks of gestation in low-middle income country: A retrospective cohort study.Contracept X. 2024 Aug 8;6:100110. doi: 10.1016/j.conx.2024.100110. eCollection 2024. Contracept X. 2024. PMID: 39281371 Free PMC article.
-
The mesoeconomics of abortion: A scoping review and analysis of the economic effects of abortion on health systems.PLoS One. 2020 Nov 4;15(11):e0237227. doi: 10.1371/journal.pone.0237227. eCollection 2020. PLoS One. 2020. PMID: 33147223 Free PMC article.
-
Cost Analysis of Surgical and Medical Uterine Evacuation Methods for First-Trimester Abortion Used in Public Hospitals in Mexico.Health Serv Insights. 2022 Sep 23;15:11786329221126347. doi: 10.1177/11786329221126347. eCollection 2022. Health Serv Insights. 2022. PMID: 36171763 Free PMC article.
-
The macroeconomics of abortion: A scoping review and analysis of the costs and outcomes.PLoS One. 2021 May 6;16(5):e0250692. doi: 10.1371/journal.pone.0250692. eCollection 2021. PLoS One. 2021. PMID: 33956826 Free PMC article.
References
-
- Republic of South Africa. No. 92 of 1996: Choice on Termination of Pregnancy Act, 1996. Pretoria, South Africa, South Africa: Cape Town: Government Printer; 1996.
-
- Harries J, Lince N, Constant D, Hargey A, Grossman D. The Challenge of Offering Public Sector Second Trimester Abortion Services in South Africa: Health care providers’ perspectives. J Biosoc Sci 2012;44:197–208. doi: 10.1017/S0021932011000678 - DOI - PubMed
-
- Harries J, Cooper D, Strebel A, Colvin CJ. Conscientious objection and its impact on abortion service provision in South Africa: a qualitative study. Reprod Health 2014;11:16 doi: 10.1186/1742-4755-11-16 - DOI - PMC - PubMed
-
- Morroni C, Myer L, Tibazarwa K. Knowledge of the abortion legislation among South African women: a cross-sectional study. Reprod Health 2006;3:7 doi: 10.1186/1742-4755-3-7 - DOI - PMC - PubMed
-
- Morroni C, Moodley J. Characteristics of women booking for first and second trimester abortions at public sector clinics in Cape Town. South African J Obstet Gynecol 2006;12:81–2.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
