

Comparison of Methods for Improving Fracture Risk Assessment in Diabetes: The Manitoba BMD Registry
- PMID: 29953670
- PMCID: PMC6193547
- DOI: 10.1002/jbmr.3538
Comparison of Methods for Improving Fracture Risk Assessment in Diabetes: The Manitoba BMD Registry
Abstract
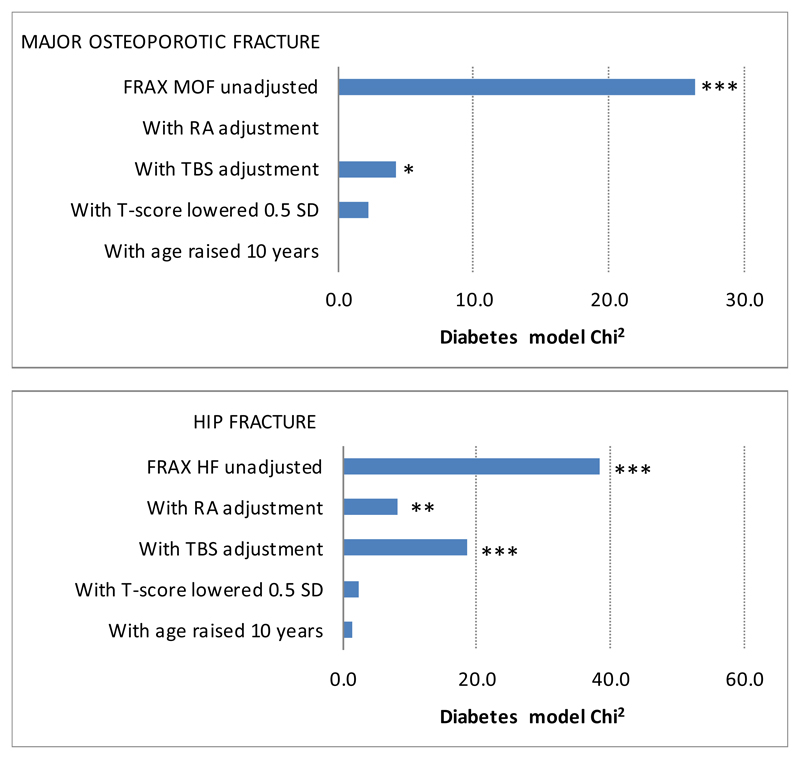
Type 2 diabetes is a risk factor for fracture independent of FRAX (fracture risk assessment) probability. We directly compared four proposed methods to improve the performance of FRAX for type 2 diabetes by: (1) including the rheumatoid arthritis (RA) input to FRAX; (2) making a trabecular bone score (TBS) adjustment to FRAX; (3) reducing the femoral neck T-score input to FRAX by 0.5 SD; and (4) increasing the age input to FRAX by 10 years. We examined major osteoporotic fractures (MOFs) and hip fractures (HFs) over a mean of 8.3 years observation among 44,543 women and men 40 years of age or older (4136 with diabetes) with baseline lumbar spine and hip DXA from 1999 through 2016. Controlled for unadjusted FRAX probability, diabetes was associated with an increased risk for MOFs and HFs. All four FRAX adjustments attenuated the effect of diabetes, but a residual effect of diabetes was seen on MOF risk after TBS adjustment, and on HF risk after the RA and TBS adjustments. Among those with diabetes, unadjusted FRAX risk underestimated MOF (observed/predicted ratio 1.15; 95% CI, 1.03 to 1.28), but this was no longer significant after applying the diabetes adjustments. HF risk was more severely underestimated (observed/predicted ratio 1.85; 95% CI, 1.51 to 2.20) and was only partially corrected with the diabetes adjustments (still significant for the RA and TBS adjustments). Among those with diabetes, there was moderate reclassification based upon a fixed MOF cut-off of 20% (4.1% to 7.1%) or fixed HF cut-off of 3% (5.7% to 16.5%). Net reclassification improvement increased for MOF with each of the diabetes adjustments (range 3.9% to 5.6% in the diabetes subgroup). In conclusion, each of the proposed methods for addressing limitations in the ability of FRAX to assess fracture risk in individuals with diabetes was found to improve performance, though no single method was optimal in all settings. © 2018 American Society for Bone and Mineral Research.
Keywords: DIABETES; DXA; FRACTURE RISK ASSESSMENT; FRAX; OSTEOPOROSIS; TRABECULAR BONE SCORE.
© 2018 American Society for Bone and Mineral Research.
Conflict of interest statement
William Leslie, Helena Johansson declare that they have no conflict of interest.
Eugene McCloskey: Nothing to declare for FRAX and the context of this paper, but numerous ad hoc consultancies/ speaking honoraria and/or research funding from Amgen, Bayer, General Electric, GSK, Hologic, Lilly, Merck Research Labs, Novartis, Novo Nordisk, Nycomed, Ono, Pfizer, ProStrakan, Roche, Sanofi-Aventis, Servier, Tethys, UBS and Warner-Chilcott.
Nicholas Harvey: Nothing to declare for FRAX and the context of this paper, but has received consultancy, lecture fees and honoraria from Alliance for Better Bone Health, AMGEN, MSD, Eli Lilly, Servier, Shire, UCB, Radius, Consilient Healthcare and Internis Pharma.
John A. Kanis: Grants from Amgen, grants from Lilly, non-financial support from Medimaps, grants from Unigene, non-financial support from Asahi, grants from Radius Health, outside the submitted work; and Dr Kanis is the architect of FRAX but has no financial interest. Governmental and NGOs: National Institute for health and clinical Excellence (NICE), UK; International Osteoporosis Foundation; INSERM, France; Ministry of Public Health, China; Ministry of Health, Australia; Ministry of Health, Abu Dhabi; National Osteoporosis Guideline Group, UK; WHO.
Didier Hans: Co-ownership in the TBS patent. Stock options or royalties: Med-Imaps. Research grants: Amgen, Radius Pharma, Agnovos, GE Healthcare.
Figures
References
-
- Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med. 1993;94(6):646–50. - PubMed
-
- Marshall D, Hailey D, Jonsson E. Health policy on bone density measurement technology in Sweden and Australia. Health Policy. 1996;35(3):217–28. - PubMed
-
- Stone KL, Seeley DG, Lui LY, Cauley JA, Ensrud K, Browner WS, et al. BMD at multiple sites and risk of fracture of multiple types: long-term results from the Study of Osteoporotic Fractures. J Bone Miner Res. 2003;18(11):1947–54. - PubMed
-
- Kanis JA. Technical Report. Published by the University of Sheffield; 2007. Assessment of osteoporosis at the primary health-care level. Accessible at http://www.shef.ac.uk/FRAX/pdfs/WHO_Technical_Report.pdf.
Publication types
MeSH terms
Grants and funding
- 17702/VAC_/Versus Arthritis/United Kingdom
- MC_U147585827/MRC_/Medical Research Council/United Kingdom
- 21231/VAC_/Versus Arthritis/United Kingdom
- 21231/ARC_/Arthritis Research UK/United Kingdom
- MC_U147585819/MRC_/Medical Research Council/United Kingdom
- 17702/ARC_/Arthritis Research UK/United Kingdom
- MC_UP_A620_1014/MRC_/Medical Research Council/United Kingdom
- MC_UU_12011/1/MRC_/Medical Research Council/United Kingdom
- HTA/10/33/04/DH_/Department of Health/United Kingdom
- G0400491/MRC_/Medical Research Council/United Kingdom
- MC_U147585824/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
