

Pneumatosis cystoides intestinalis: six case reports and a review of the literature
- PMID: 29954324
- PMCID: PMC6022295
- DOI: 10.1186/s12876-018-0794-y
Pneumatosis cystoides intestinalis: six case reports and a review of the literature
Abstract
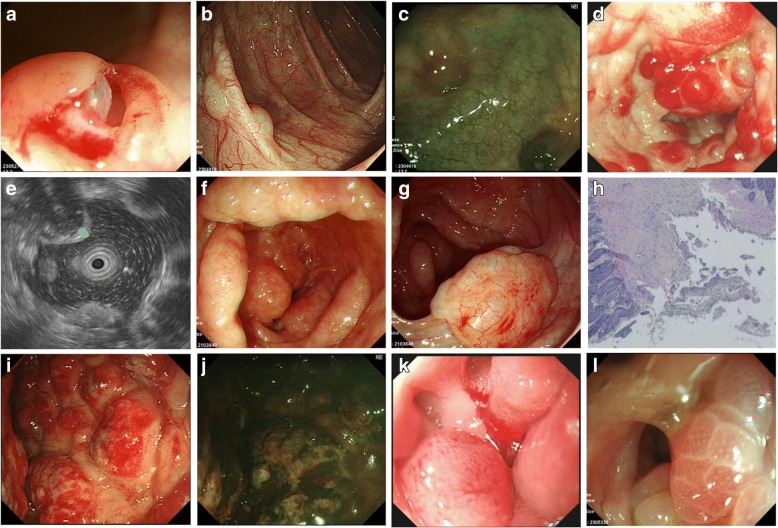
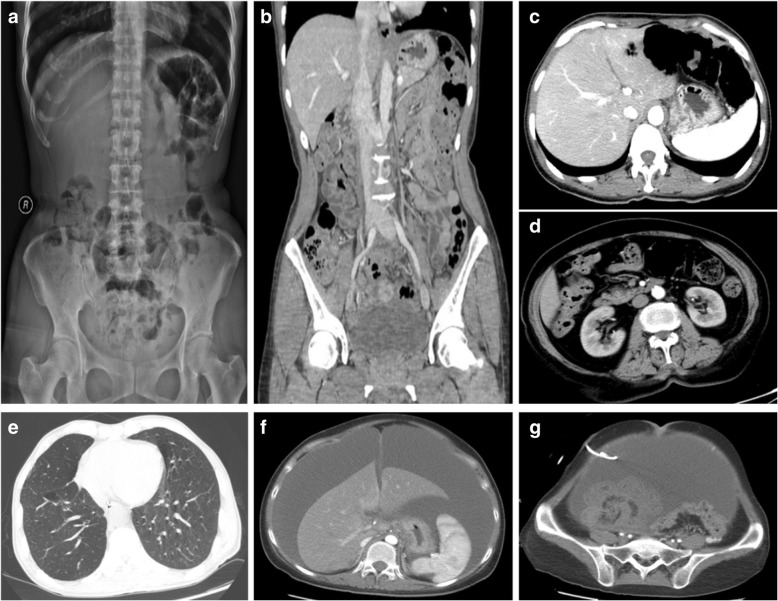
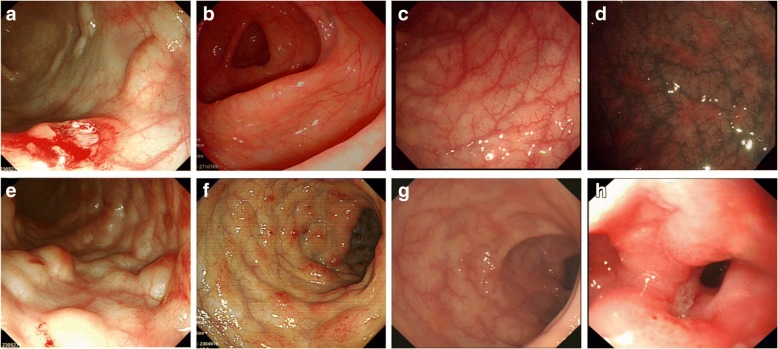
Background: Pneumatosis cystoides intestinalis (PCI) is characterized by gas-filled cysts in the intestinal submucosa and subserosa. There are few reports of PCI occurring in duodenum and rectum. Here we demonstrated four different endoscopic manifestations of PCI and three cases with intestinal stricture all were successfully managed by medical conservative treatment.
Case presentation: There are 6 cases of PCI with varied causes encountered, in which the etiology, endoscopic features, treatment methods and prognosis of patients were studied. One case was idiopathic, while the other one case was caused by exposing to trichloroethylene (TCE), and the remaining four cases were secondary to diabetes, emphysema, therioma and diseases of immune system. Of the six patients, all complained of abdominal distention or diarrhea, three (50%) reported muco-bloody stools, two (33.3%) complained of abdominal pain. In four other patients, PCI occurred in the colon, especially the sigmoid colon, while in the other two patients, it occurred in duodenum and rectum. Endoscopic findings were divided into bubble-like pattern, grape or beaded circular forms, linear or cobblestone gas formation and irregular forms. After combination of medicine and endoscopic treatment, the symptoms of five patients were relieved, while one patient died of malignant tumors.
Conclusion: PCI endoscopic manifestations were varied, and radiology combined with endoscopy can avoid misdiagnosis. The primary bubble-like pattern can be cured by endoscopic resection, while removal of etiology combined with drug therapy can resolve majority of secondary cases, thereby avoiding the adverse risks of surgery.
Keywords: Diagnosis; Endoscopy; Pneumatosis Cystoides intestinalis; Therapy.
Conflict of interest statement
Ethics approval and consent to participate
This article is a retrospective study and does not contain any studies with human subjects performed by any of the authors. So, the ethical approval was not necessary and the General Hospital of Tianjin Medical University medical ethics committee can offer exempt ethical statement in support.
Consent for publication
Written informed consent was obtained from the patients for publication of this case reports and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Heng Y, Schuffler MD, Haggitt RC, Rohrmann CA. Pneumatosis intestinalis: a review. Am J Gastroenterol. 1995;90:1747–1758. - PubMed
-
- KOSS LG. Abdominal gas cysts (pneumatosis cystoides intestinorum hominis); an analysis with a report of a case and a critical review of the literature. AMA Arch Pathol. 1952;53(6):523–549. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
