

Cytomegalovirus infection and outcome in immunocompetent patients in the intensive care unit: a systematic review and meta-analysis
- PMID: 29954328
- PMCID: PMC6027797
- DOI: 10.1186/s12879-018-3195-5
Cytomegalovirus infection and outcome in immunocompetent patients in the intensive care unit: a systematic review and meta-analysis
Abstract
Background: Cytomegalovirus (CMV) infection is common in immunocompetent patients in intensive care units (ICUs). However, whether CMV infection or CMV reactivation contributes to mortality of immunocompetent patients remains unclear.
Methods: A literature search was conducted for relevant studies published before May 30, 2016. Studies reporting on CMV infection in immunocompetent patients in ICUs and containing 2 × 2 tables on CMV results and all-cause mortality were included.
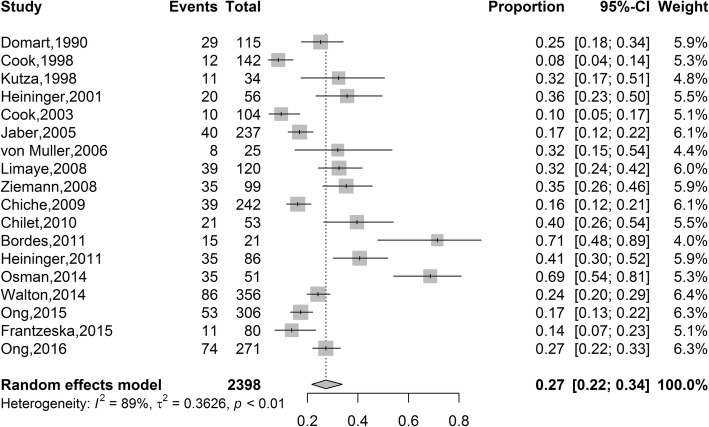
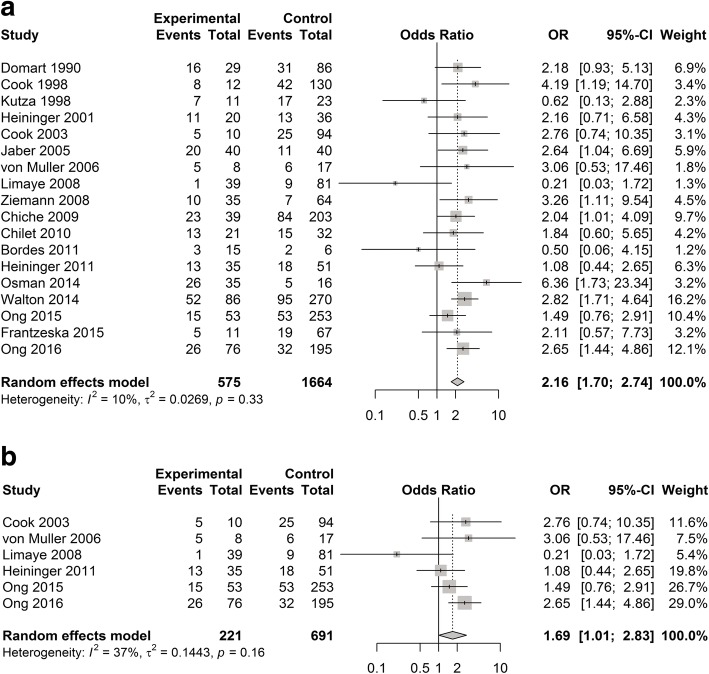
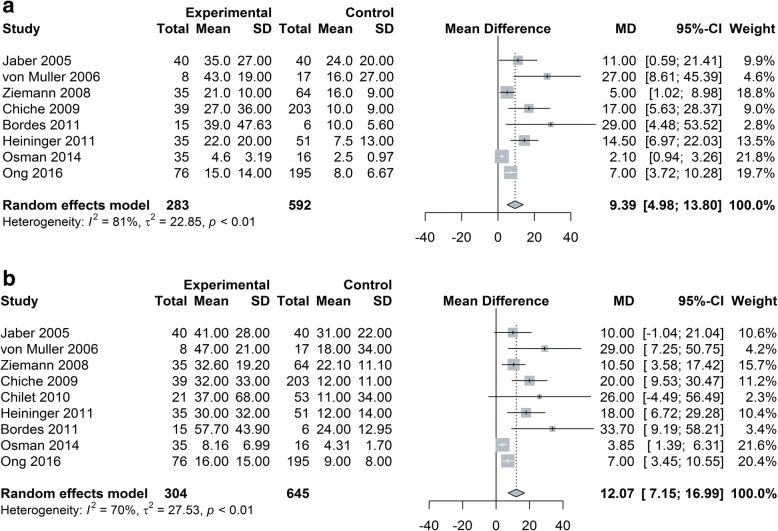
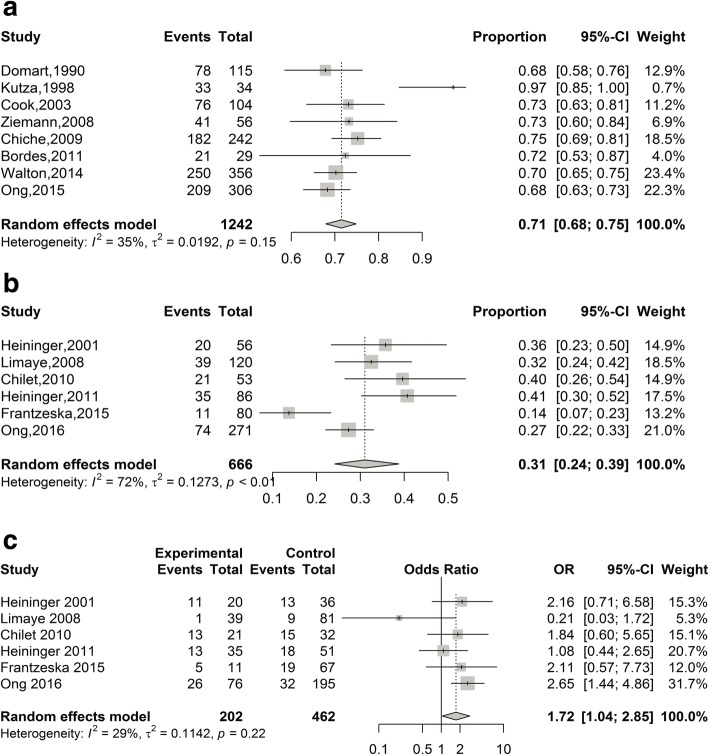
Results: Eighteen studies involving 2398 immunocompetent patients admitted to ICUs were included in the meta-analysis. The overall rate of CMV infection was 27% (95%CI 22-34%, I2 = 89%, n = 2398) and the CMV reactivation was 31% (95%CI 24-39%, I2 = 74%, n = 666). The odds ratio (OR) for all-cause mortality among patients with CMV infection, compared with those without infection, was 2.16 (95%CI 1.70-2.74, I2 = 10%, n = 2239). Moreover, upon exclusion of studies in which antiviral treatment was possibly or definitely provided to some patients, the association of mortality rate with CMV infection was also statistically significant (OR: 1.69, 95%CI 1.01-2.83, I2 = 37%, n = 912,). For CMV seropositive patients, the OR for mortality in patients with CMV reactivation as compared with patients without CMV reactivation was 1.72 (95%CI 1.04-2.85, I2 = 29%, n = 664). Patients with CMV infection required significantly longer mechanical ventilation (mean difference (MD): 9 days (95% CI 5-14, I2 = 81%, n = 875)) and longer duration of ICU stay (MD: 12 days (95% CI 7-17, I2 = 70%, n = 949)) than patients without CMV infection. When analysis was limited to detection in blood, CMV infection without antiviral drug treatment or reactivation was not significantly associated with higher mortality (OR: 1.69, 95%CI 0.81-3.54, I2 = 52%, n = 722; OR: 1.49, I2 = 63%, n = 469).
Conclusion: Critically ill patients without immunosuppression admitted to ICUs show a high rate of CMV infection. CMV infection during the natural unaltered course or reactivation in critically ill patients is associated with increased mortality, but have no effect on mortality when CMV in blood. More studies are needed to clarify the impact of CMV infection on clinical outcomes in those patients.
Keywords: Cytomegalovirus; Immunocompetent; Meta-analysis.
Conflict of interest statement
Ethics approval and consent to participate
This review evaluated data from published studies and was exempt from ethics committee approval. This review did not involve any direct research on patients, and no informed consent was required.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
