

Risk factors for complications and mortality of percutaneous endoscopic gastrostomy insertion
- PMID: 29954339
- PMCID: PMC6025834
- DOI: 10.1186/s12876-018-0825-8
Risk factors for complications and mortality of percutaneous endoscopic gastrostomy insertion
Abstract
Background: Percutaneous endoscopic gastrostomy (PEG) is a relatively safe procedure; however, acute and chronic complications of PEG have been reported. We aimed to determine risk factors associated with complications and 30-day mortality after PEG, based on 11 years of experience at a single tertiary hospital.
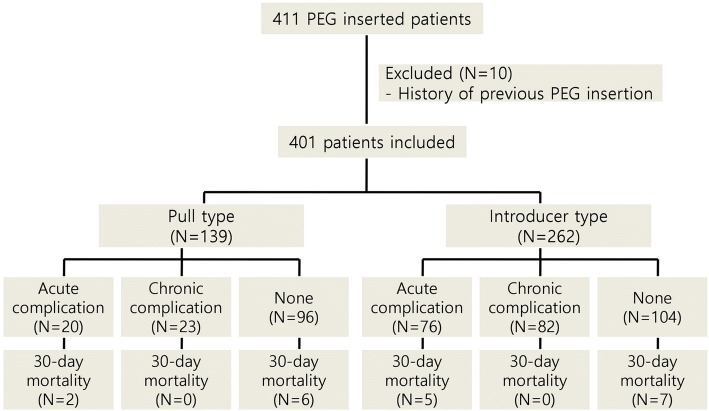
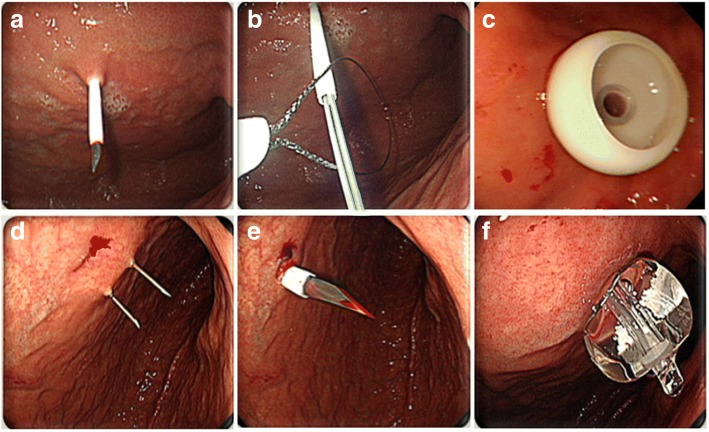
Methods: In total, 401 patients who underwent first PEG insertion at the Asan Medical Center, Seoul, Korea, between January 2005 and December 2015 were eligible. Medical records were retrospectively reviewed to determine clinical characteristics and outcomes of 139 and 262 patients who underwent pull-type and introducer-type PEG, respectively.
Results: The median age of the overall population was 68 years, and the median body mass index was 19.5 kg/m2. Acute and chronic complications developed in 96 (23.9%) and 105 (26.2%) patients. Acute ileus and chronic tube obstruction were significantly more frequent in the introducer-type PEG group (p = 0.033 and 0.001, respectively). The 30-day mortality rate was 5.0% (median survival: 10.5 days). Multivariate analysis revealed that underlying malignancy was a predictor of acute complications; age ≥ 70 years and diabetes mellitus were predictors of chronic complications. The median follow-up was 354 days. Neurologic disease and malignancy were the most common indications for PEG. Neurologic diseases were classified into two groups: stroke and the other neurologic disease group (including dementia, Parkinson's disease, neuromuscular disease, and hypoxic brain damage). Multivariate analysis showed that 30-day mortality was significantly lower in the other neurologic disease group and higher in patients with platelet count < 100,000/μL, and C-reactive protein (CRP) ≥ 5 mg/dL.
Conclusions: PEG is a relatively safe and feasible procedure, but it was associated with significantly higher early mortality rate in patients with platelet count < 100,000/μL or CPR≥5mg/dL, and lower early mortality rate in neurologic disease group including dementia, Parkinson's disase, neuromuscular disease, and hypoxic brain damage. In addition, acute complications in patients with underlying malignancy, and chronic complications in patients aged ≥70 and those with diabetes mellitus should be considered during and after PEG.
Keywords: Complication; Endoscopy; Gastrostomy; Mortality; Stomach.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved and authorized by the hospital’s ethical committee (Asan Medical Center). Ethical approval number: 2017–1399. The consent of patients was waived by the hospital’s ethical committee.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Gauderer MW, Ponsky JL, Izant RJ, Jr.: Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg 1980, 15(6):872–875. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
