

INvestigation on Routine Follow-up in CONgestive HearT FAilure Patients with Remotely Monitored Implanted Cardioverter Defibrillators SysTems (InContact)
- PMID: 29954340
- PMCID: PMC6025705
- DOI: 10.1186/s12872-018-0864-7
INvestigation on Routine Follow-up in CONgestive HearT FAilure Patients with Remotely Monitored Implanted Cardioverter Defibrillators SysTems (InContact)
Abstract
Background: In heart failure (HF) patients with implantable cardioverter defibrillators (ICD) or cardiac resynchronisation therapy defibrillators (CRT-D), remote monitoring has been shown to result in at least non-inferior outcomes relative to in-clinic visits. We aimed to provide further evidence for this effect, and to assess whether adding telephone follow-ups to remote follow-ups influenced outcomes.
Methods: InContact was a prospective, randomised, multicentre study. Subjects receiving quarterly automated follow-up only (telemetry group) were compared to those receiving personal physician contact. Personal contact patients were further divided into those receiving automated follow-up plus a telephone call (remote+phone subgroup) or in-clinic visits only.
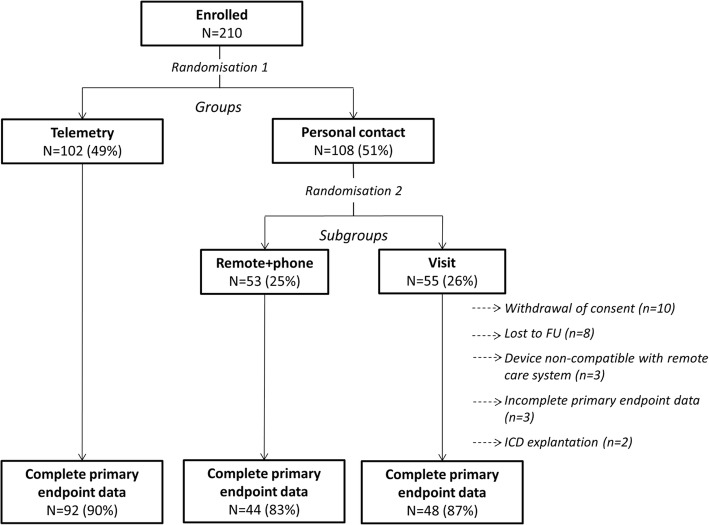
Results: Two hundred and ten patients underwent randomisation (telemetry n = 102; personal contact n = 108 [remote+phone: n = 53; visit: n = 55]). Baseline characteristics were comparable between groups and subgroups. Over 12 months, 34.8% of patients experienced deterioration of their Packer Clinical Composite Response, with no significant difference between the telemetry group and personal care (p > 0.999), remote+phone (p = 0.937) or visit (p = 0.940) patients; predefined non-inferiority criteria were met. Mortality rates (5.2% overall) were comparable between groups and subgroups (p = 0.832/p = 0.645), as were HF-hospitalisation rates (11.0% overall; p = 0.605/p = 0.851). The proportion of patients requiring ≥1 unscheduled follow-up was nominally higher in telemetry and remote+phone groups (42.2 and 45.3%) compared to the visit group (29.1%). Overall, ≥ 1 ICD therapy was delivered to 15.2% of patients.
Conclusion: In HF patients with ICDs/CRT-Ds, quarterly remote follow-up only over 12 months was non-inferior to regular personal contact. Addition of quarterly telephone follow-ups to remote monitoring does not appear to offer any clinical advantage.
Trial registration: clinicaltrials.gov: NCT01200381 (retrospectively registered on September 13th 2010).
Keywords: Cardiac resynchronisation therapy defibrillator; Heart failure; Implantable cardioverter defibrillator; Packer heart failure clinical composite response; Remote monitoring.
Conflict of interest statement
Ethics approval and consent to participate
The protocol was approved by the relevant ethics committees and the study was carried out in accordance with the Declaration of Helsinki 1964 and its amendments. All patients provided written informed consent.
Ethic Committee of the Medical Facultry, University of Göttingen: Göttingen, Lüneburg.
Ethic Committee International Freiburg: Bad Friedrichshall, Cologne, Stuttgart, Sindelfingen, Potsdam, Ludwigsburg, Bielefeld, Essen, Nürtingen.
Ethic Committee of the Bavarian Medical Association: Ingolstadt.
Ethic Committee of the Hamburg Medical Association: Hamburg.
Ethic Committee of the Schleswig Holstein Medical Association: Bad Segeberg, Bad Oldesloe.
Ethic Committee of the Rhineland Palatinate Medical Association: Neuwied.
Consent for publication
Not applicable.
Competing interests
Peter Bramlage has received honoraria relevant to this topic. Frank Birkenhauer is an employee of Abbott. The other authors have no competing interest to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, et al. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol. 2014;63(12):1123–1133. doi: 10.1016/j.jacc.2013.11.053. - DOI - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Drazner MH, et al. ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147–e239. doi: 10.1016/j.jacc.2013.05.019. - DOI - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891–975. doi: 10.1002/ejhf.592. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
