

Successful emergent repair of a subacute left ventricular free wall rupture after acute inferoposterolateral myocardial infarction
- PMID: 29954429
- PMCID: PMC6025822
- DOI: 10.1186/s13019-018-0764-z
Successful emergent repair of a subacute left ventricular free wall rupture after acute inferoposterolateral myocardial infarction
Abstract
Background: Myocardial rupture is an important and catastrophic complication of acute myocardial infarction. A dramatic form of this complication is a left ventricular free wall rupture (LVFWR).
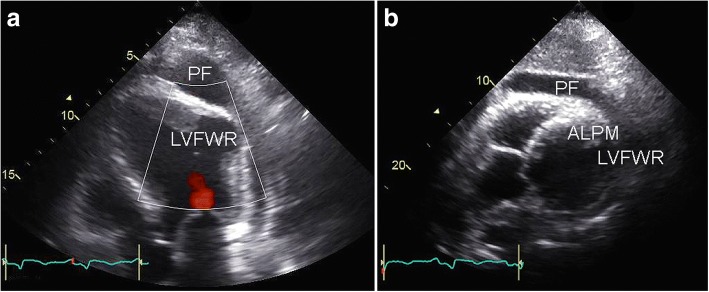
Case presentation: A 70-year-old man with acute inferoposterolateral myocardial infarction and single-vessel coronary artery disease underwent emergency percutaneous coronary intervention (PCI). The circumflex coronary artery was successfully stented with a drug-eluting stent. Fifty days after PCI the patient experienced progressive fatigue and chest pain with haemodynamic instability. Transthoracic echocardiography showed a covered LVFWR of the lateral wall. The patient underwent successful emergent surgical repair of the LVFWR.
Conclusions: In the current era of swift PCI, mechanical complications of acute myocardial infarction, such as LVFWR, are rare. The consequences, however, are haemodynamic deterioration and imminent death. This rare diagnosis should always be considered when new cardiovascular symptoms or haemodynamic instability develop after myocardial infarction, even beyond one month after the initial event. Timely diagnosis and emergency surgery are required for successful treatment of this devastating complication.
Keywords: Myocardial infarction, heart rupture, percutaneous coronary intervention, cardiac surgical procedures.
Conflict of interest statement
Consent for publication
Informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
