

Presentation, Clinical Profile, and Prognosis of Young Patients With Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): Results From the VIRGO Study
- PMID: 29954744
- PMCID: PMC6064896
- DOI: 10.1161/JAHA.118.009174
Presentation, Clinical Profile, and Prognosis of Young Patients With Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): Results From the VIRGO Study
Abstract
Background: We compared the clinical characteristics and outcomes of young patients with myocardial infarction with nonobstructive coronary arteries (MINOCA) versus obstructive disease (myocardial infarction due to coronary artery disease [MI-CAD]) and among patients with MINOCA by sex and subtype.
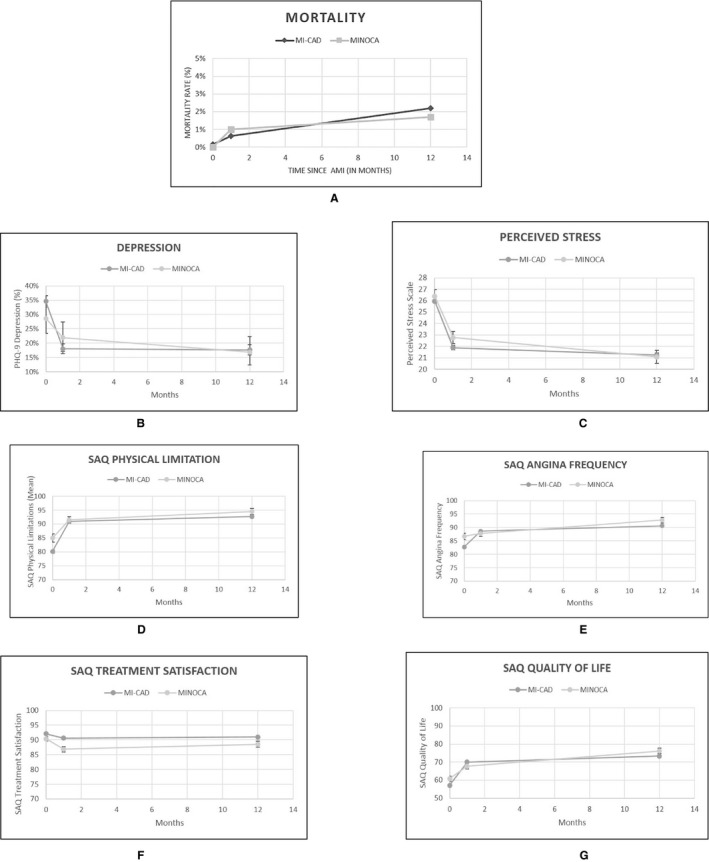
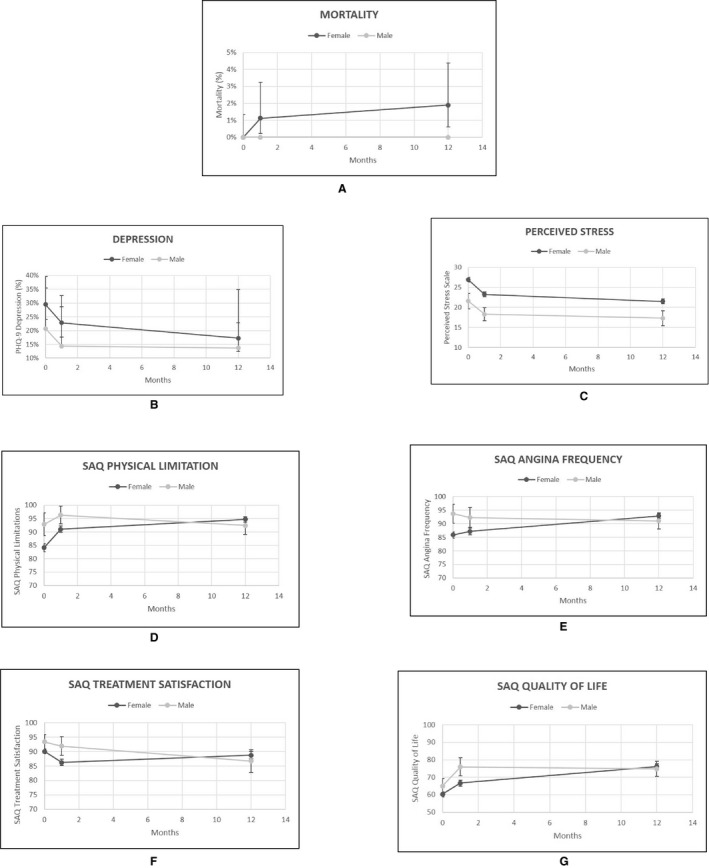
Methods and results: Between 2008 and 2012, VIRGO (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients) prospectively enrolled acute myocardial infarction patients aged 18 to 55 years in 103 hospitals at a 2:1 ratio of women to men. Using an angiographically driven taxonomy, we defined patients as having MI-CAD if there was revascularization or plaque ≥50% and as having MINOCA if there was <50% obstruction or a nonplaque mechanism. Patients who did not have an angiogram or who received thrombolytics before an angiogram were excluded. Outcomes included 1- and 12-month mortality and functional (Seattle Angina Questionnaire [SAQ]) and psychosocial status. Of 2690 patients undergoing angiography, 2374 (88.4%) had MI-CAD, 299 (11.1%) had MINOCA, and 17 (0.6%) remained unclassified. Women had 5 times higher odds of having MINOCA than men (14.9% versus 3.5%; odds ratio: 4.84; 95% confidence interval, 3.29-7.13). MINOCA patients were more likely to be without traditional cardiac risk factors (8.7% versus 1.3%; P<0.001) but more predisposed to hypercoaguable states than MI-CAD patients (3.0% versus 1.3%; P=0.036). Women with MI-CAD were more likely than those with MINOCA to be menopausal (55.2% versus 41.2%; P<0.001) or to have a history of gestational diabetes mellitus (16.8% versus 11.0%; P=0.028). The MINOCA mechanisms varied: a nonplaque mechanism was identified for 75 patients (25.1%), and their clinical profiles and management also varied. One- and 12-month mortality with MINOCA and MI-CAD was similar (1-month: 1.1% and 1.7% [P=0.43]; 12-month: 0.6% and 2.3% [P=0.68], respectively), as was adjusted 12-month SAQ quality of life (76.5 versus 73.5, respectively; P=0.06).
Conclusions: Young patients with MINOCA were more likely women, had a heterogeneous mechanistic profile, and had clinical outcomes that were comparable to those of MI-CAD patients.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00597922.
Keywords: acute myocardial infarction; myocardial infarction with nonobstructive coronary arteries; nonobstructive; prognosis; sex; women.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Comment in
-
Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): It's Time to Face Reality!J Am Heart Assoc. 2018 Jun 28;7(13):e009635. doi: 10.1161/JAHA.118.009635. J Am Heart Assoc. 2018. PMID: 29954745 Free PMC article. No abstract available.
References
-
- Beltrame JF. Assessing patients with myocardial infarction and nonobstructed coronary arteries (MINOCA). J Intern Med. 2013;273:182–185. - PubMed
-
- DeWood MA, Spores J, Notske R, Mouser LT, Burroughs R, Golden MS, Lang HT. Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction. N Engl J Med. 1980;303:897–902. - PubMed
-
- Patel MR, Chen AY, Peterson ED, Newby LK, Pollack CV Jr, Brindis RG, Gibson CM, Kleiman NS, Saucedo JF, Bhatt DL, Gibler WB, Ohman EM, Harrington RA, Roe MT. Prevalence, predictors, and outcomes of patients with non–ST‐segment elevation myocardial infarction and insignificant coronary artery disease: results from the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines (CRUSADE) initiative. Am Heart J. 2006;152:641–647. - PubMed
-
- Dokainish H, Pillai M, Murphy SA, DiBattiste PM, Schweiger MJ, Lotfi A, Morrow DA, Cannon CP, Braunwald E, Lakkis N; TACTICS‐TIMI‐18 Investigators . Prognostic implications of elevated troponin in patients with suspected acute coronary syndrome but no critical epicardial coronary disease: a TACTICS‐TIMI‐18 substudy. J Am Coll Cardiol. 2005;45:19–24. - PubMed
-
- Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015;131:861–870. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
