

Hepatic epithelioid angiomyolipoma with renal metastasis: radiologic-pathologic correlation
- PMID: 29955240
- PMCID: PMC6020097
- DOI: 10.1016/j.radcr.2018.05.007
Hepatic epithelioid angiomyolipoma with renal metastasis: radiologic-pathologic correlation
Abstract
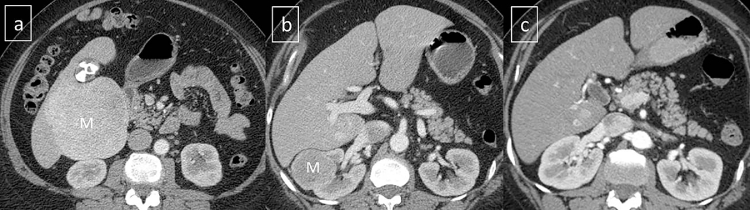
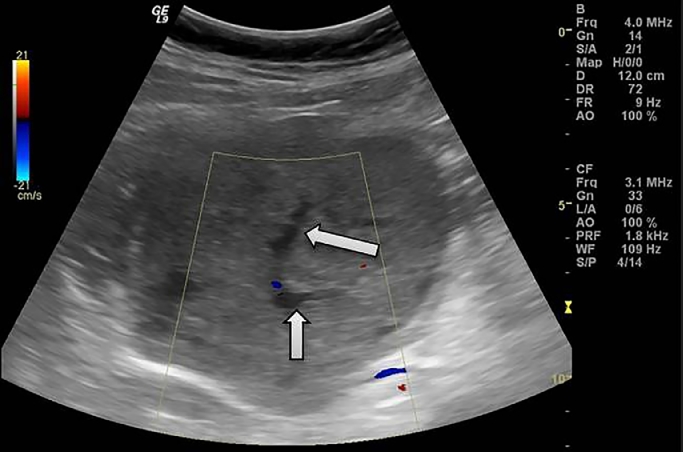
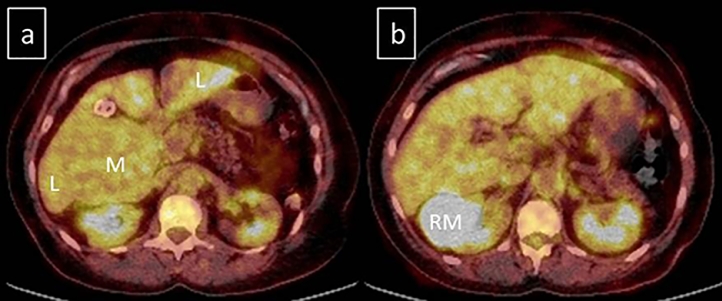
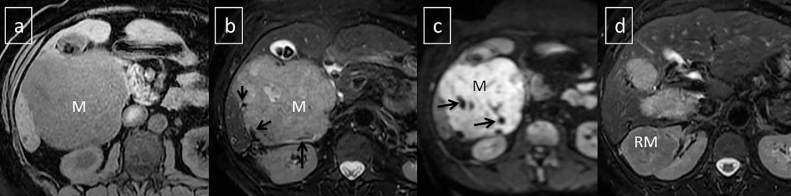
Epithelioid angiomyolipoma (EAML) is a rare subtype of angiomyolipomas. Unlike the conventional angiomyolipomas, EAML often contains minimal fat which usually precludes prospective diagnosis on imaging. The imaging findings of EAML may overlap with other benign and malignant hepatic neoplasms. We report a hepatic epithelioid angiomyolipoma in a 47-year-old female which metastasized to the right kidney and recurred after resection in the liver. We analyze the imaging findings of EAML on ultrasound, computed tomography, positron emission tomography and magnetic resonance imaging. Correlation between the imaging and histopathologic findings is made. The estimated annual growth and doubling time of the primary hepatic EAML are calculated. To the best of our knowledge, this is the first published report of positron emission tomography-computed tomography findings and annual growth rate for hepatic EAML.
Keywords: Epithelioid angiomyolipoma; Liver PET.
Figures


Similar articles
-
Renal epithelioid angiomyolipoma: computed tomography manifestation and radiologic-pathologic correlation depending on different epithelioid component percentages.Abdom Radiol (NY). 2022 Jan;47(1):310-319. doi: 10.1007/s00261-021-03313-3. Epub 2021 Oct 19. Abdom Radiol (NY). 2022. PMID: 34664098
-
Hepatic epithelioid angiomyolipoma: a report of two cases and review of the literature.Int J Clin Exp Pathol. 2018 Mar 1;11(3):1739-1745. eCollection 2018. Int J Clin Exp Pathol. 2018. PMID: 31938278 Free PMC article.
-
Malignant renal epithelioid angiomyolipoma with liver metastasis after resection: a case report with multimodality imaging and review of the literature.J Comput Assist Tomogr. 2014 Jul-Aug;38(4):574-7. doi: 10.1097/RCT.0000000000000101. J Comput Assist Tomogr. 2014. PMID: 24887578 Review.
-
Renal epithelioid angiomyolipoma: imaging characteristics in nine cases with radiologic-pathologic correlation and review of the literature.AJR Am J Roentgenol. 2013 Feb;200(2):W178-86. doi: 10.2214/AJR.12.8776. AJR Am J Roentgenol. 2013. PMID: 23345382 Review.
-
Clinical and pathological features of renal epithelioid angiomyolipoma (PEComa): A single institution series.Urol Oncol. 2022 Feb;40(2):18-24. doi: 10.1016/j.urolonc.2021.09.010. Epub 2021 Nov 20. Urol Oncol. 2022. PMID: 34815169 Review.
Cited by
-
Elevated 18F-FDG accumulation in a malignant epithelioid angiomyolipoma: a case report and review of literature.Front Oncol. 2025 Apr 16;15:1555092. doi: 10.3389/fonc.2025.1555092. eCollection 2025. Front Oncol. 2025. PMID: 40308494 Free PMC article.
-
Metastases to the Kidney: A Case Report and Review of the Literature.Curr Health Sci J. 2020 Jan-Mar;46(1):80-89. doi: 10.12865/CHSJ.46.01.11. Epub 2020 Mar 31. Curr Health Sci J. 2020. PMID: 32637169 Free PMC article.
-
Clinical characteristics and outcomes of patients with hepatic angiomyolipoma: A literature review.World J Gastroenterol. 2021 May 21;27(19):2299-2311. doi: 10.3748/wjg.v27.i19.2299. World J Gastroenterol. 2021. PMID: 34040323 Free PMC article. Review.
References
-
- Xiao W, Zhou M, Lou H, Wang Z, Zhang M. Hemodynamic characterization of hepatic angiomyolipoma with least amount of fat evaluated by contrast-enhanced magnetic resonance angiography. Abdom Imaging. 2010 Apr 1;35(2):203–207. - PubMed
-
- Dalle I, Sciot R, De Vos R, Aerts R, Van Damme B, Desmet V. Malignant angiomyolipoma of the liver: a hitherto unreported variant. Histopathology. 2000 May 1;36(5):443–450. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
