

Neurotrophic Keratopathy after Trigeminal Nerve Block for Treatment of Postherpetic Neuralgia
- PMID: 29955409
- PMCID: PMC6000878
- DOI: 10.1155/2018/6815407
Neurotrophic Keratopathy after Trigeminal Nerve Block for Treatment of Postherpetic Neuralgia
Abstract
Purpose: To report a case of persistent corneal epithelial defect that had occurred after a trigeminal nerve block.
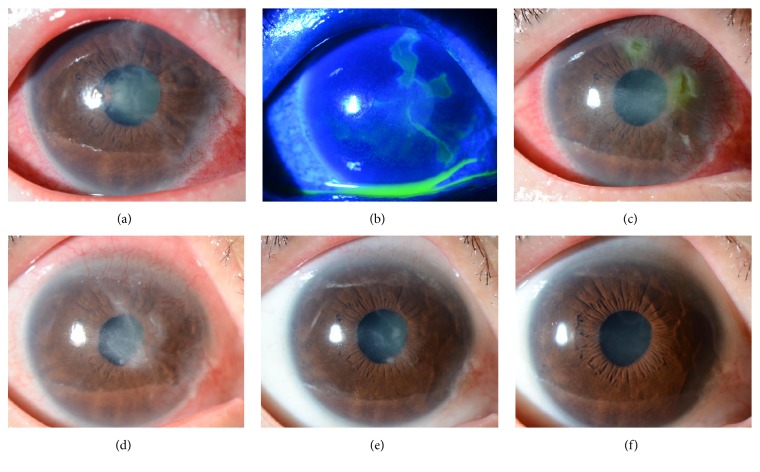
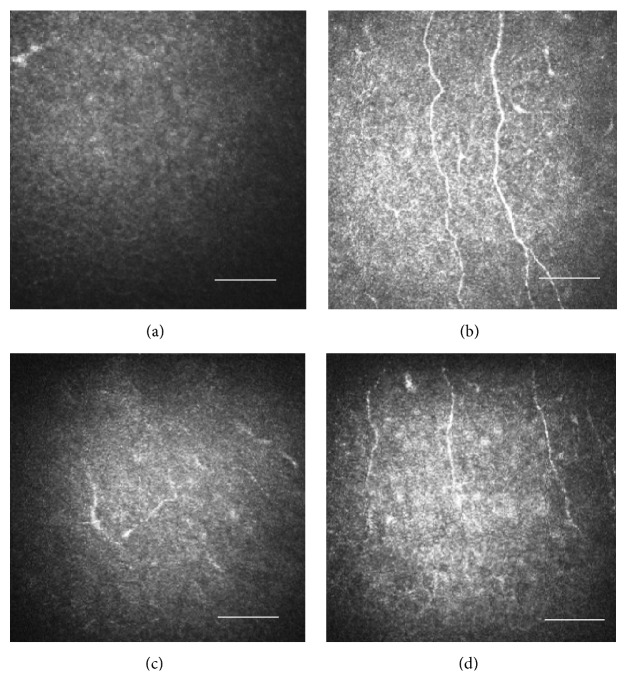
Case presentation: A 75-year-old female had suffered from postherpetic neuralgia for 8 years. She underwent Gasserian ganglion block surgery and noticed declining visual acuity in the right eye on the following day. She presented with severe hyperemia and corneal epithelial defects in the right eye and experienced remarkable reduction of sensitivity in the right cornea. She was diagnosed with neurotrophic keratopathy. Ofloxacin eye ointment and rebamipide ophthalmic suspension ameliorated the corneal epithelial defects but superficial punctate keratopathy, corneal superficial neovascularization, and Descemet's fold persisted. Although the epithelial defects occasionally recurred, the corneal sensation and epithelial defects, Descemet's fold, and corneal superficial neovascularization all improved around 5 months after trigeminal nerve block. The HRT II Rostock Cornea Module (RCM) could not detect any corneal subbasal nerve fibers at postoperative 4 months; however, it could detect them at postoperative 6 months.
Conclusions: As the nerve block effect wore off, the corneal subbasal nerve fibers slowly regenerated. As the corneal sensation improved, the corneal epithelial defects and superficial neovascularization also improved. The HRT II RCM appeared useful for observing loss and regeneration of the corneal subbasal nerve fibers.
Figures
References
-
- Okada Y., Reinach P. S., Kitano A., et al. Neurotrophic keratopathy; its pathophysiology and treatment. Histol Histopathol. 2010;25(6):771–80. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
