

Arthroscopic Bone Graft Procedure Combined With Arthroscopic Subscapularis Augmentation for Recurrent Anterior Instability With Glenoid Bone Defect
- PMID: 29955568
- PMCID: PMC6020248
- DOI: 10.1016/j.eats.2018.02.009
Arthroscopic Bone Graft Procedure Combined With Arthroscopic Subscapularis Augmentation for Recurrent Anterior Instability With Glenoid Bone Defect
Abstract
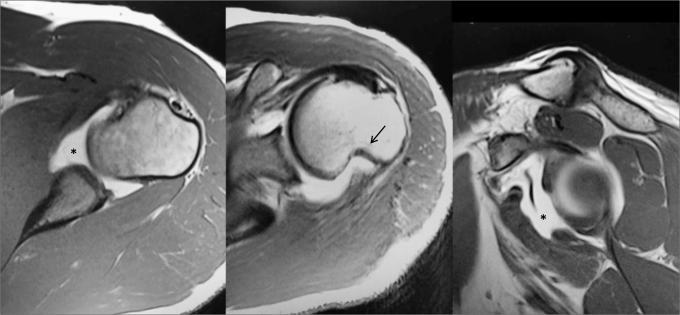
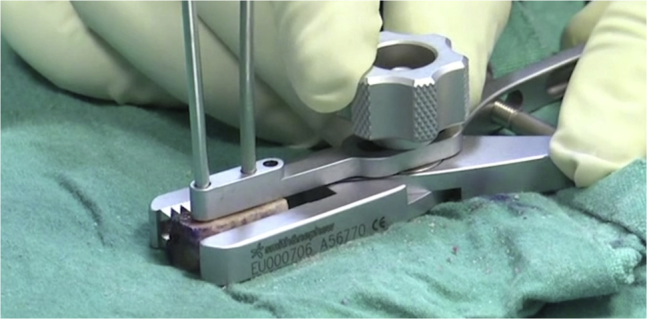
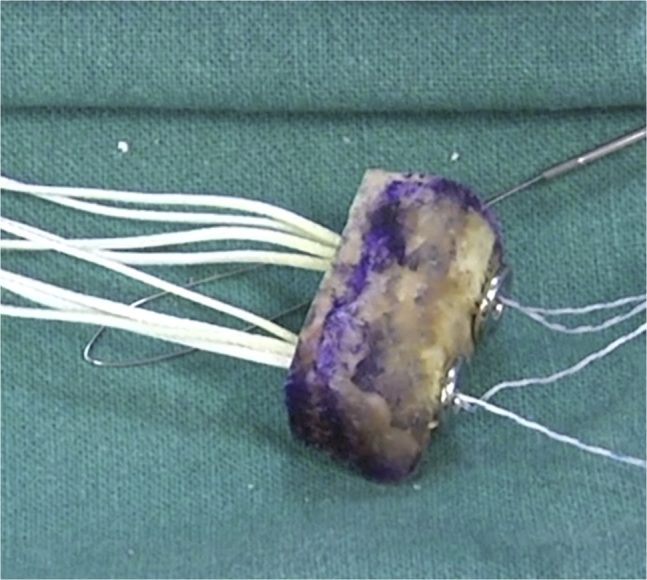
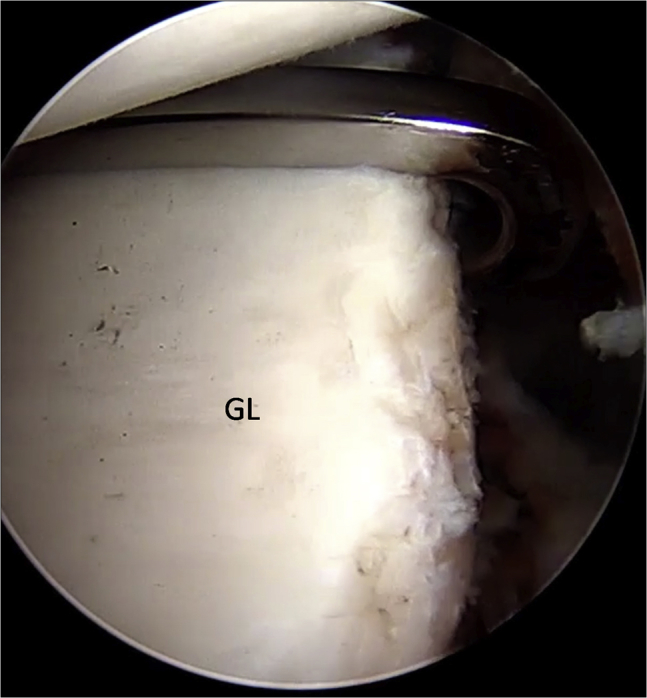
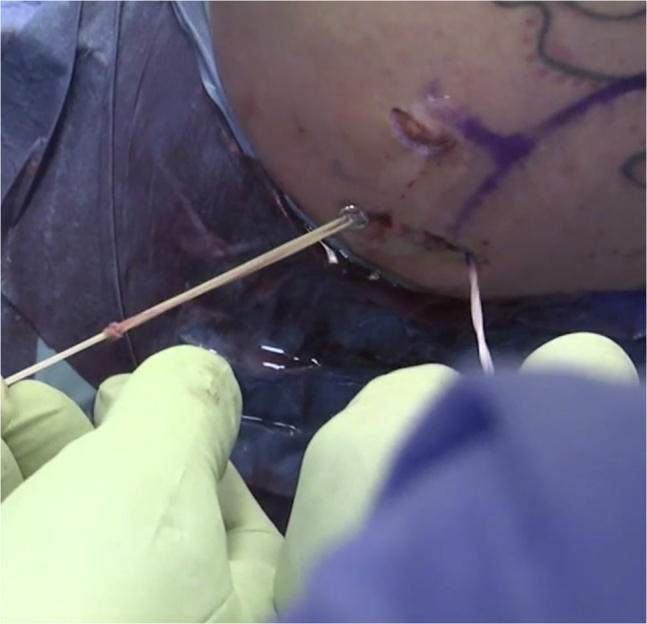
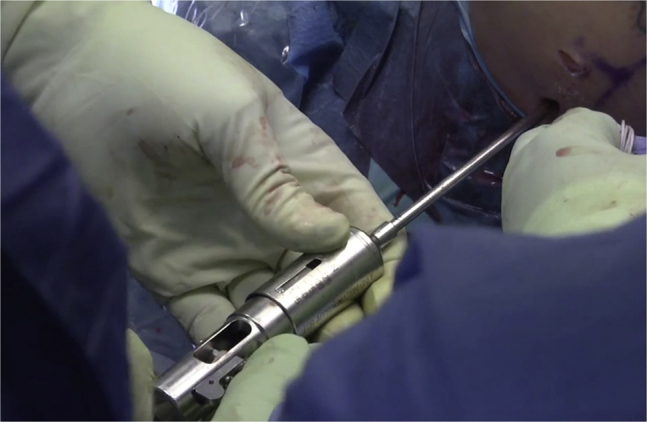
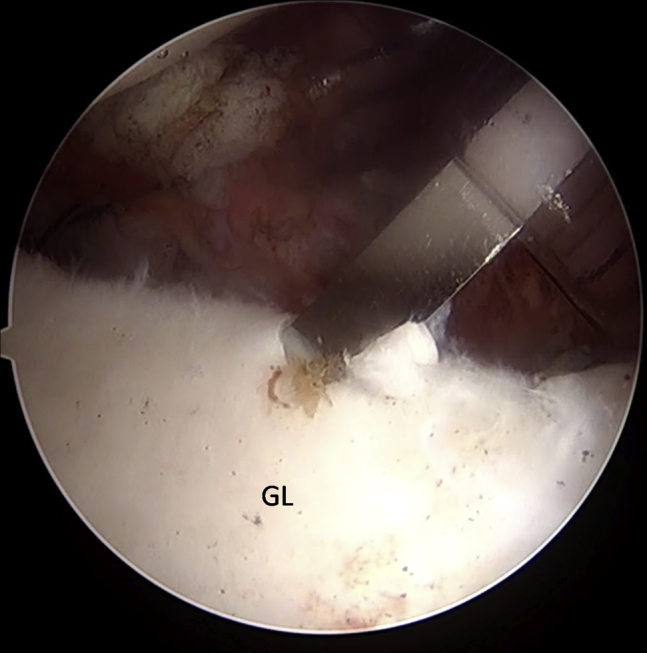
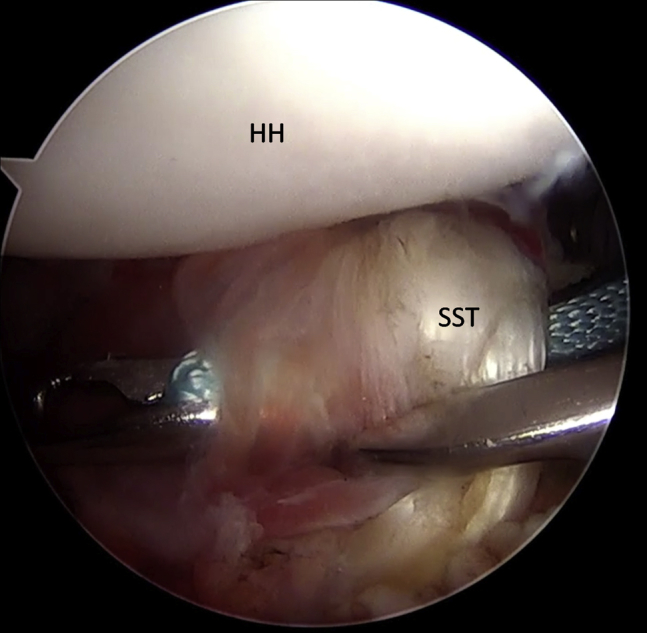
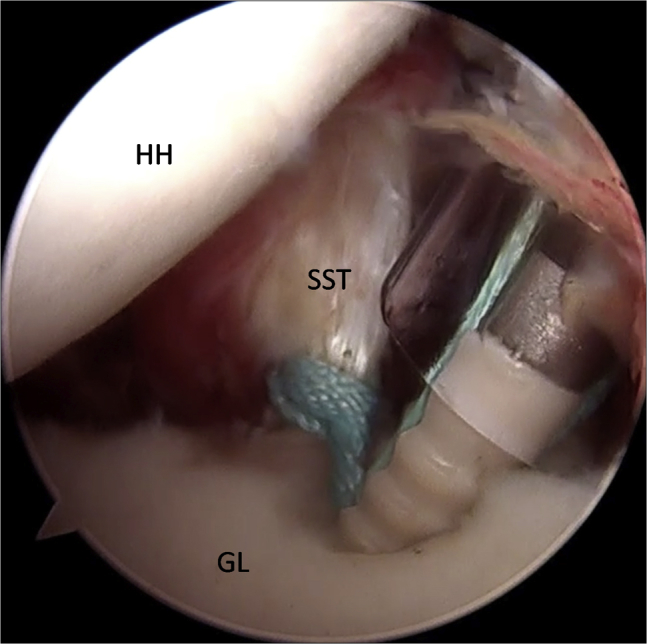
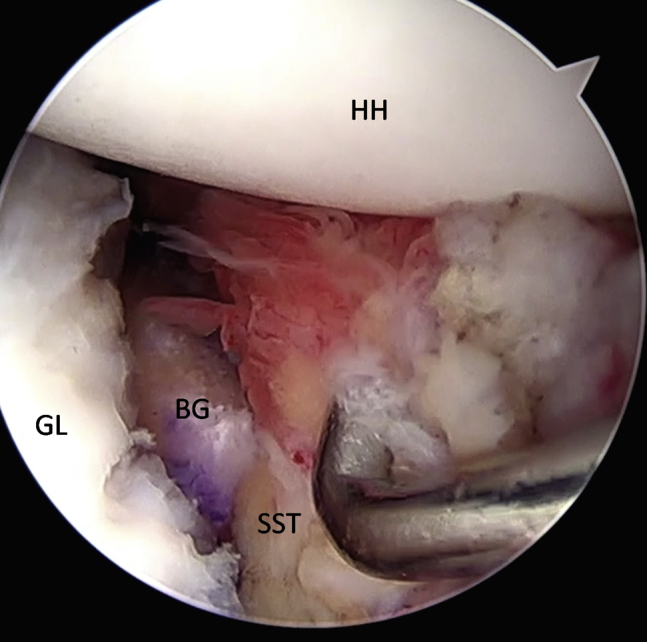
Glenoid bone loss and capsular deficiency represent critical points of arthroscopic Bankart repair failures. The purpose of this Technical Note is to present an all-arthroscopic bone block procedure associated with arthroscopic subscapularis augmentation for treating glenohumeral instability with glenoid bone loss and anterior capsulolabral deficiency. Two glenoid tunnels are set up from the posterior to the anterior side using a dedicated bone block guide, and 4 buttons are used to fix the graft to the glenoid. The subscapularis tenodesis is performed using a suture tape anchor. This combined arthroscopic technique (bone block associated with arthroscopic subscapularis augmentation) could be a valid and safe alternative to the arthroscopic or open Latarjet procedures.
Figures




References
-
- Alkaduhimi H., van der Linde J.A., Willigenburg N.W., Paulino Pereira N.R., van Deurzen D.F., van den Bekerom M.P. Redislocation risk after an arthroscopic Bankart procedure in collision athletes: A systematic review. J Shoulder Elbow Surg. 2016;25:1549–1558. - PubMed
-
- Arciero R.A., Parrino A., Bernhardson A.S. The effect of a combined glenoid and Hill-Sachs defect on glenohumeral stability: A biomechanical cadaveric study using 3-dimensional modeling of 142 patients. Am J Sports Med. 2015;43:1422–1429. - PubMed
-
- Burkhart S.S., De Beer J.F. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16:677–694. - PubMed
-
- Di Giacomo G., de Gasperis N., Scarso P. Bipolar bone defect in the shoulder anterior dislocation. Knee Surg Sports Traumatol Arthrosc. 2016;24:479–488. - PubMed
-
- Shin S.J., Koh Y.W., Bui C. What is the critical value of glenoid bone loss at which soft tissue Bankart repair does not restore glenohumeral translation, restricts range of motion, and leads to abnormal humeral head position? Am J Sports Med. 2016;44:2784–2791. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
