

Vitamin D in the Middle East and North Africa
- PMID: 29955632
- PMCID: PMC6020111
- DOI: 10.1016/j.bonr.2018.03.004
Vitamin D in the Middle East and North Africa
Abstract
Purpose: The Middle East and North Africa (MENA) region registers some of the lowest serum 25‑hydroxyvitamin D [25(OH)D] concentrations, worldwide. We describe the prevalence and the risk factors for hypovitaminosis D, completed and ongoing clinical trials, and available guidelines for vitamin D supplementation in this region.
Methods: This review is an update of previous reviews published by our group in 2013 for observational studies, and in 2015 for randomized controlled trials (RCTs) from the region. We conducted a comprehensive search in Medline, PubMed, and Embase, and the Cochrane Library, using MeSH terms and keywords relevant to vitamin D, vitamin D deficiency, and the MENA region, for the period 2012-2017 for observational studies, and 2015-2017 for RCTs. We included large cross-sectional studies with at least 100 subjects/study, and RCTs with at least 50 participants per arm.
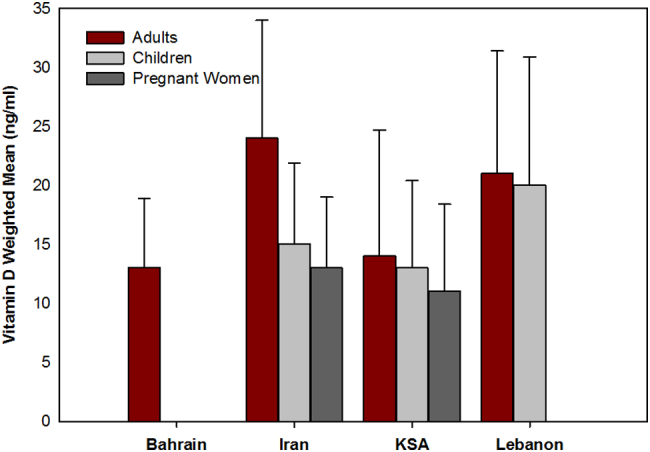
Results: We identified 41 observational studies. The prevalence of hypovitaminosis D, defined as a 25‑hydroxyvitamin D [25(OH)D] level below the desirable level of 20 ng/ml, ranged between 12-96% in children and adolescents, and 54-90% in pregnant women. In adults, it ranged between 44 and 96%, and the mean 25(OH)D varied between 11 and 20 ng/ml. In general, significant predictors of low 25(OH)D levels were female gender, increasing age and body mass index, veiling, winter season, use of sun screens, lower socioeconomic status, and higher latitude.We retrieved 14 RCTs comparing supplementation to control or placebo, published during the period 2015-2017: 2 in children, 8 in adults, and 4 in pregnant women. In children and adolescents, a vitamin D dose of 1000-2000 IU/d was needed to maintain serum 25(OH)D level at target. In adults and pregnant women, the increment in 25(OH)D level was inversely proportional to the dose, ranging between 0.9 and 3 ng/ml per 100 IU/d for doses ≤2000 IU/d, and between 0.1 and 0.6 ng/ml per 100 IU/d for doses ≥3000 IU/d. While the effect of vitamin D supplementation on glycemic indices is still controversial in adults, vitamin D supplementation may be protective against gestational diabetes mellitus in pregnant women. In the only identified study in the elderly, there was no significant difference between 600 IU/day and 3750 IU/day doses on bone mineral density. We did not identify any fracture studies.The available vitamin D guidelines in the region are based on expert opinion, with recommended doses between 400 and 2000 IU/d, depending on the age category, and country.
Conclusion: Hypovitaminosis D is prevalent in the MENA region, and doses of 1000-2000 IU/d may be necessary to reach a desirable 25(OH)D level of 20 ng/ml. Studies assessing the effect of such doses of vitamin D on major outcomes, and confirming their long term safety, are needed.
Keywords: 25(OH)D, 25‑hydroxyvitamin D; ALKP, alkaline phosphatase; BMC, bone mineral content; BMD, bone mineral density; BMI, body mass index; CARS, Childhood Autism Rating Scale; CDC, Centers for Disease Control; Ca, Calcium; DEQAS, Vitamin D External Quality Assessment Scheme; DXA, dual-energy X-ray absorptiometry; ESCEO, European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis; GDM, Gestational Diabetes Mellitus; HOMA-IR, homeostatic model assessment of insulin resistance; HbA1c, glycated hemoglobin; Hypovitaminosis D; ID LC-MS/MS, isotope dilution liquid chromatography - tandem mass spectrometry; IOM, Institute of Medicine; KSA, Kingdom of Saudi Arabia; LCMS/MS, liquid chromatography-tandem mass spectrometry; MENA, Middle East North Africa; Middle East and North Africa; OSTEOS, Lebanese Society for Osteoporosis and Metabolic Bone Disorders; PO4, phosphorus; PTH, parathyroid hormone; Predictors; RCT, randomized controlled trials; ROB, risk of bias; RR, relative risk; SDp, pooled standard deviation; T2D, type 2 diabetes; UAE, United Arab Emirates; UVB, ultraviolet B; VDDR2, vitamin d dependent rickets type 2; VDR, vitamin d receptor; VDSP, Vitamin D Standardization Program; Vitamin D assays; Vitamin D guidelines; WM, weighted mean.
Figures
References
-
- Akbari M., Mosazadeh M., Lankarani K.B. The effects of vitamin D supplementation on glucose metabolism and lipid profiles in patients with gestational diabetes: a systematic review and meta-analysis of randomized controlled trials. Horm. Metab. Res. 2017;49(9):647–653. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
