

Comparing Survival Outcomes and Costs Associated With Radical Cystectomy and Trimodal Therapy for Older Adults With Muscle-Invasive Bladder Cancer
- PMID: 29955780
- PMCID: PMC6584312
- DOI: 10.1001/jamasurg.2018.1680
Comparing Survival Outcomes and Costs Associated With Radical Cystectomy and Trimodal Therapy for Older Adults With Muscle-Invasive Bladder Cancer
Abstract
Importance: Radical cystectomy is the guidelines-recommended treatment of muscle-invasive bladder cancer, but a resurgence of trimodal therapy has occurred. Limited comparative data are available on outcomes and costs attributable to these 2 treatments.
Objective: To compare the survival outcomes and costs between trimodal therapy and radical cystectomy in older adults with muscle-invasive bladder cancer.
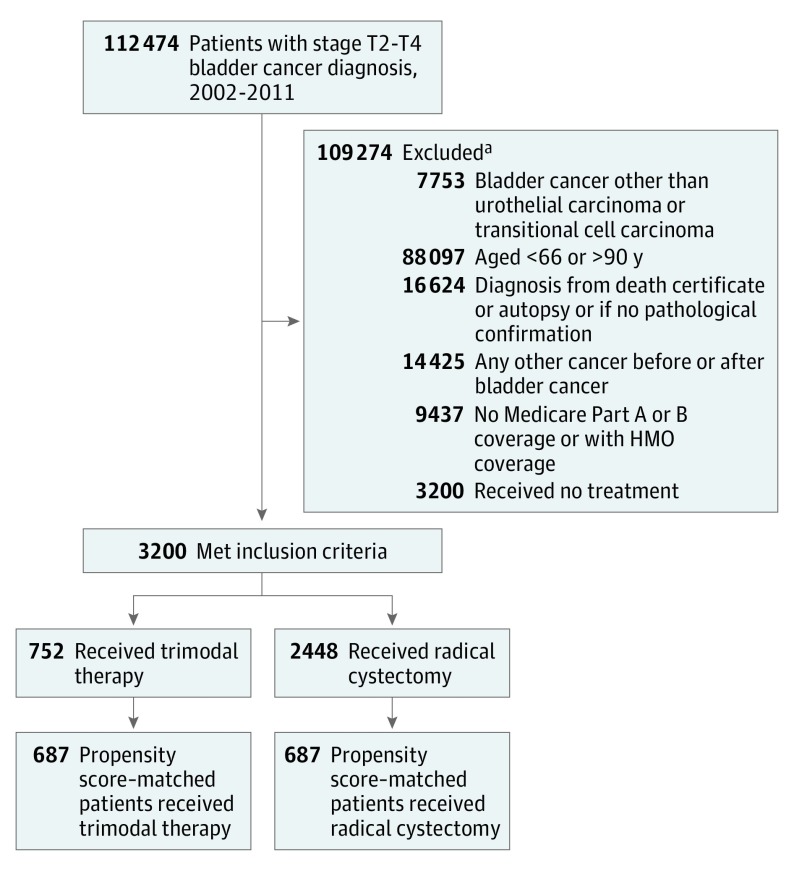
Design, setting, and participants: This population-based cohort study used data from the Surveillance, Epidemiology, and End Results-Medicare linked database. A total of 3200 older adults (aged ≥66 years) with clinical stage T2 to T4a bladder cancer diagnosed from January 1, 2002, to December 31, 2011, and with claims data available through December 31, 2013, were included in the analysis. Patients who received radical cystectomy underwent either only surgery or surgery in combination with radiotherapy or chemotherapy. Patients who received trimodal therapy underwent transurethral resection of the bladder followed by radiotherapy and chemotherapy. Propensity score matching by sociodemographic and clinical characteristics was used. Data analysis was performed from August 1, 2017, to March 11, 2018.
Main outcomes and measures: Overall survival and cancer-specific survival were evaluated using the Cox proportional hazards regression model and the Fine and Gray competing risk model. All Medicare health care costs for inpatient, outpatient, and physician services within 30, 90, and 180 days of treatment were compared. The total amount spent nationwide was estimated, using 180-day medical costs between treatments, by the total number of new cases of muscle-invasive bladder cancer in the United States in 2011.
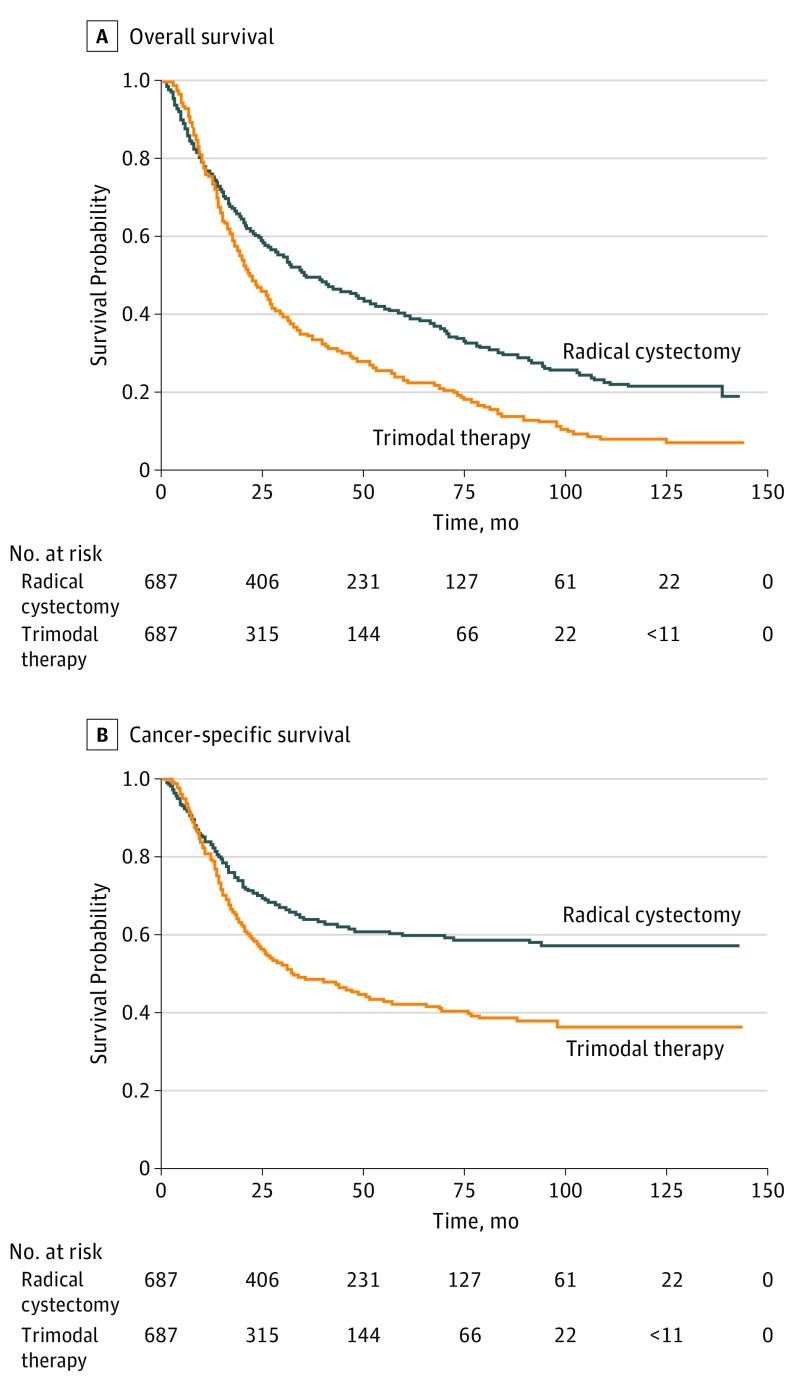
Results: Of the 3200 patients who met the inclusion criteria, 2048 (64.0%) were men and 1152 (36.0%) were women, with a mean (SD) age of 75.8 (6.0) years. After propensity score matching, 687 patients (21.5%) underwent trimodal therapy and 687 patients (21.5%) underwent radical cystectomy. Patients who underwent trimodal therapy had significantly decreased overall survival (hazard ratio [HR], 1.49; 95% CI, 1.31-1.69) and cancer-specific survival (HR, 1.55; 95% CI, 1.32-1.83). No differences in costs at 30 days were observed between trimodal therapy ($15 233 in 2002 vs $18 743 in 2011) and radical cystectomy ($17 990 in 2002 vs $21 738 in 2011). However, median total costs were significantly higher with trimodal therapy than with radical cystectomy at 90 days ($80 174 vs $69 181; median difference, $8964; Hodges-Lehmann 95% CI, $3848-$14 079) and at 180 days ($179 891 vs $107 017; median difference, $63 771; Hodges-Lehmann 95% CI, $55 512-$72 029). Extrapolating these figures to the total US population revealed $335 million in excess spending for trimodal therapy compared with the less costly radical cystectomy ($492 million) for patients who received a muscle-invasive bladder cancer diagnosis in 2011.
Conclusions and relevance: Trimodal therapy was associated with significantly decreased overall survival and cancer-specific survival as well as $335 million in excess spending in 2011. These findings have important health policy implications regarding the appropriate use of high value-based care among older adults with invasive bladder cancer who are candidates for either radical cystectomy or trimodal therapy.
Conflict of interest statement
Figures
Comment in
-
Bladder Extirpation vs Preservation: The Treatment Debate.JAMA Surg. 2018 Oct 1;153(10):889-890. doi: 10.1001/jamasurg.2018.1674. JAMA Surg. 2018. PMID: 29955758 No abstract available.
-
Utility of Bladder-Sparing Therapy vs Radical Cystectomy for Muscle-Invasive Bladder Cancer-Reply.JAMA Surg. 2019 Feb 1;154(2):186. doi: 10.1001/jamasurg.2018.4372. JAMA Surg. 2019. PMID: 30476959 No abstract available.
-
Utility of Bladder-Sparing Therapy vs Radical Cystectomy for Muscle-Invasive Bladder Cancer.JAMA Surg. 2019 Feb 1;154(2):185-186. doi: 10.1001/jamasurg.2018.4371. JAMA Surg. 2019. PMID: 30477005 No abstract available.
-
Utility of Bladder-Sparing Therapy vs Radical Cystectomy for Muscle-Invasive Bladder Cancer.JAMA Surg. 2019 Feb 1;154(2):184-185. doi: 10.1001/jamasurg.2018.4370. JAMA Surg. 2019. PMID: 30477011 No abstract available.
-
Re: Comparing Survival Outcomes and Costs Associated with Radical Cystectomy and Trimodal Therapy for Older Adults with Muscle-Invasive Bladder Cancer.J Urol. 2019 May;201(5):837. doi: 10.1097/01.JU.0000553996.66966.57. J Urol. 2019. PMID: 30747883 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
