

Association of the Video Head Impulse Test With Improvement of Dynamic Balance and Fall Risk in Patients With Dizziness
- PMID: 29955786
- PMCID: PMC6143005
- DOI: 10.1001/jamaoto.2018.0650
Association of the Video Head Impulse Test With Improvement of Dynamic Balance and Fall Risk in Patients With Dizziness
Abstract
Importance: It is important to know whether recovery of the vestibuloocular reflex (VOR) as measured by the video head impulse test (vHIT) is associated with the recovery of dynamic balance. It is also critical to know how much change in VOR gain is clinically relevant for establishing the recovery of dynamic balance.
Objectives: To investigate the association between improved VOR gain as measured by the vHIT and improved dynamic balance (reduced fall risk) as measured by the dynamic gait index (DGI) and to calculate the minimal clinically important difference of VOR gain.
Design, setting, and participants: This retrospective case series study was performed at a tertiary referral center at the Johns Hopkins University School of Medicine. Thirty-eight consecutive patients with subacute or chronic dizziness from January 1, 2014, through May 31, 2017, who visited the vestibular physical therapy clinic were included in the study.
Interventions: Each patient was evaluated with room light and video-infrared oculomotor examination, vHIT, and balance testing before and after vestibular physical therapy.
Main outcomes and measures: Gain of the lesioned VOR and score on the DGI.
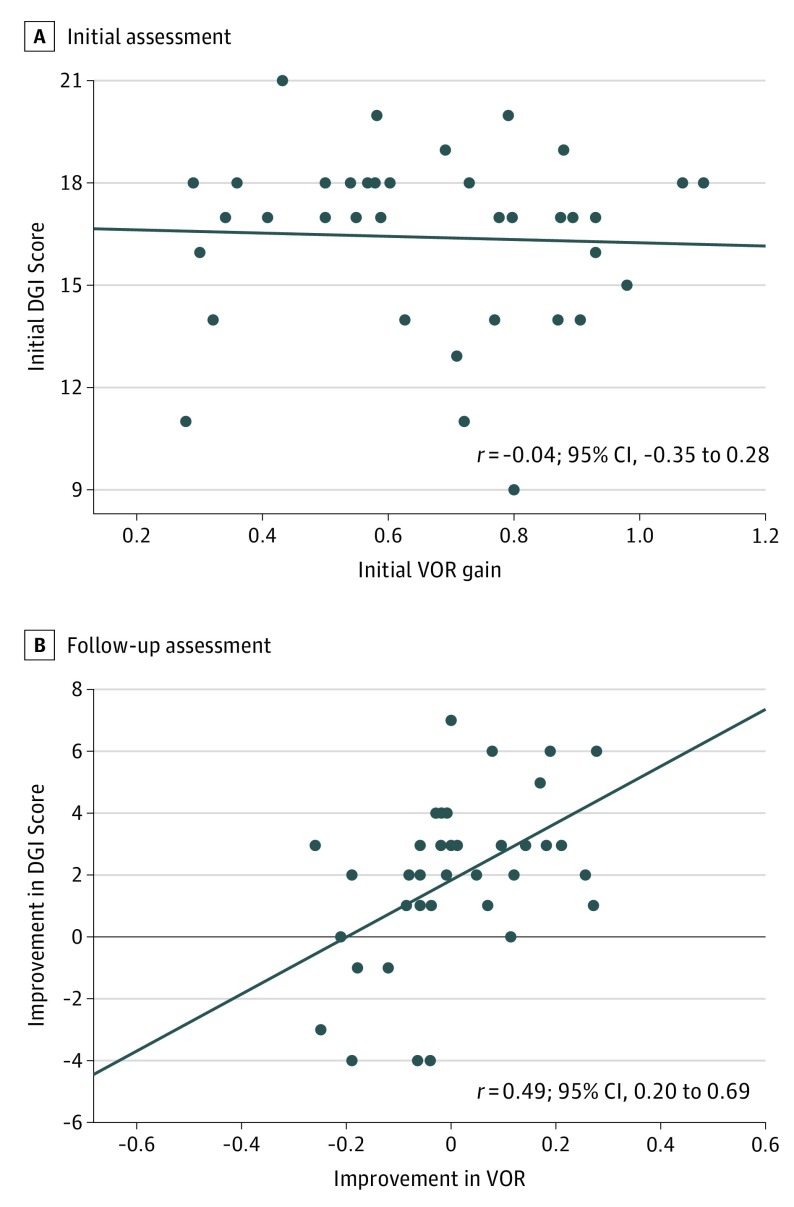
Results: Among the 38 patients (25 women [66%]; mean [SD] age, 65 [14] years), the mean (SD) initial lesioned VOR gain was 0.66 (0.23) and initial DGI score was 16 (3). No correlation was found between initial VOR gain and initial DGI score (r = -0.04; 95% CI, -0.35 to 0.28). At follow-up, 15 patients (39%) had an improved VOR gain and 30 (79%) had an improved DGI score, which was correlated (r = 0.49; 95% CI, 0.20-0.69). In those 15 patients with improved VOR gain, 14 (93%) had improvement of DGI score. In the 23 patients without improvement of VOR gain, 16 (70%) still showed improvement in their DGI score. When using VOR gain to estimate improvement of DGI, the minimal clinically important difference of VOR gain was -0.06.
Conclusions and relevance: The change of VOR gain in the vHIT was moderately associated with the change of DGI score. Improved VOR gain was associated with a high probability of improved dynamic balance. However, in most of the patients whose VOR gains did not improve, balance improvement occurred putatively through sensory reweighting strategies.
Conflict of interest statement
Figures
Similar articles
-
The usefulness of the video head impulse test in children and adults post-concussion.J Vestib Res. 2016;26(5-6):439-446. doi: 10.3233/VES-160598. J Vestib Res. 2016. PMID: 28262647
-
The map of dizziness in vestibular schwannoma.Laryngoscope. 2015 Dec;125(12):2784-9. doi: 10.1002/lary.25402. Epub 2015 Jun 18. Laryngoscope. 2015. PMID: 26086320
-
Vestibulo-Ocular Reflex Function in Adolescents With Sport-Related Concussion: Preliminary Results.Sports Health. 2019 Nov/Dec;11(6):479-485. doi: 10.1177/1941738119865262. Epub 2019 Aug 14. Sports Health. 2019. PMID: 31411942 Free PMC article.
-
Physical therapy for persons with vestibular disorders.Curr Opin Neurol. 2015 Feb;28(1):61-8. doi: 10.1097/WCO.0000000000000162. Curr Opin Neurol. 2015. PMID: 25514252 Review.
-
Video head impulse test: a review of the literature.Eur Arch Otorhinolaryngol. 2017 Mar;274(3):1215-1222. doi: 10.1007/s00405-016-4157-4. Epub 2016 Jun 21. Eur Arch Otorhinolaryngol. 2017. PMID: 27328962 Review.
Cited by
-
Gaze stabilisation exercises in vestibular rehabilitation: review of the evidence and recent clinical advances.J Neurol. 2019 Sep;266(Suppl 1):11-18. doi: 10.1007/s00415-019-09459-x. Epub 2019 Aug 5. J Neurol. 2019. PMID: 31385017 Review.
-
Improvement After Vestibular Rehabilitation Not Explained by Improved Passive VOR Gain.Front Neurol. 2020 Feb 20;11:79. doi: 10.3389/fneur.2020.00079. eCollection 2020. Front Neurol. 2020. PMID: 32153490 Free PMC article.
-
VOR gain of lateral semicircular canal using video head impulse test in acute unilateral vestibular hypofunction: A systematic review.Front Neurol. 2022 Dec 8;13:948462. doi: 10.3389/fneur.2022.948462. eCollection 2022. Front Neurol. 2022. PMID: 36570452 Free PMC article.
-
Measuring Vestibular Contributions to Age-Related Balance Impairment: A Review.Front Neurol. 2021 Feb 9;12:635305. doi: 10.3389/fneur.2021.635305. eCollection 2021. Front Neurol. 2021. PMID: 33633678 Free PMC article. Review.
-
The Identification of Elderly People with High Fall Risk Using Machine Learning Algorithms.Healthcare (Basel). 2022 Dec 23;11(1):47. doi: 10.3390/healthcare11010047. Healthcare (Basel). 2022. PMID: 36611508 Free PMC article.
References
-
- Mantokoudis G, Schubert MC, Tehrani ASS, Wong AL, Agrawal Y. Early adaptation and compensation of clinical vestibular responses after unilateral vestibular deafferentation surgery. Otol Neurotol. 2014;35(1):148-154. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
