

Characteristics and Outcomes of Surgical Patients With Solid Cancers Admitted to the Intensive Care Unit
- PMID: 29955801
- PMCID: PMC6233642
- DOI: 10.1001/jamasurg.2018.1571
Characteristics and Outcomes of Surgical Patients With Solid Cancers Admitted to the Intensive Care Unit
Abstract
Importance: Within the surgical population admitted to intensive care units (ICUs), cancer is a common condition. However, clinicians can be reluctant to admit patients with cancer to ICUs owing to concerns about survival.
Objective: To compare the clinical characteristics and outcomes of surgical patients with and without cancer who are admitted to ICUs.
Design, setting, and participants: An observational retrospective cohort study using ICU audit records linked to hospitalization discharge summaries, cancer registrations, and death records of all 16 general adult ICUs in the West of Scotland was conducted. All 25 017 surgical ICU admissions between January 1, 2000, and December 31, 2011, were included, and data analysis was conducted during that time.
Exposures: Patients were dichotomized based on a diagnosis of a solid malignant tumor as determined by its documentation in the Scottish Cancer Registry within the 2 years prior to ICU admission.
Main outcomes and measures: Intensive care unit patients with cancer were compared with ICU patients without cancer in terms of patient characteristics (age, sex, severity of illness, reason for admission, and organ support) and survival (ICU, hospital, 6 months, and 4 years).
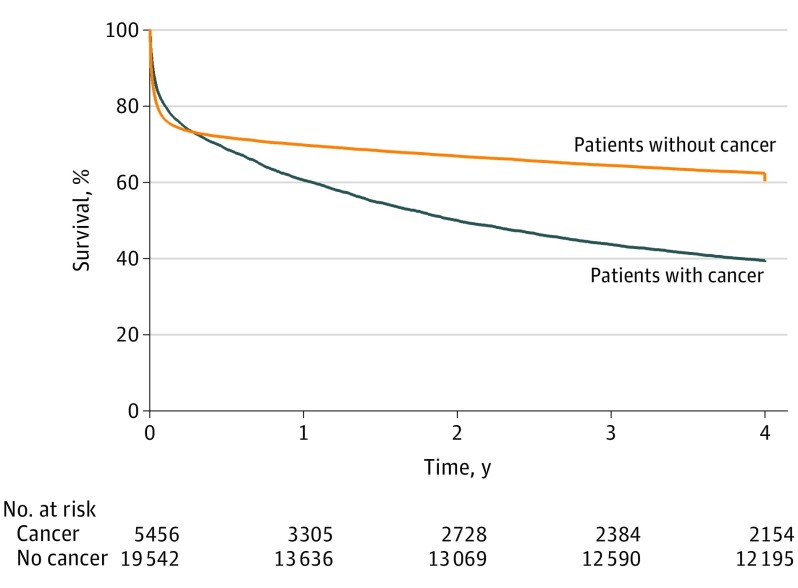
Results: Within the 25 017 surgical ICU patients, 13 684 (54.7%) were male, the median (interquartile range [IQR]) age was 64 (50-74), and 5462 (21.8%) had an underlying solid tumor diagnosis. Patients with cancer were older (median [IQR] age, 68 [60-76] vs 62 [45-74] years; P < .001) with a higher proportion of elective hospitalizations (60.5% vs 19.8%; P < .001), similar Acute Physiology and Chronic Health Evaluation II scores (median for both, 17), but lower use of multiorgan support (57.9% vs 66.7%; P < .001). Intensive care unit and hospital mortality were lower for the cancer group, at 12.2% (95% CI, 11.3%-13.1%) vs 16.8% (95% CI, 16.3%-17.4%) (P < .001) and 22.9% (95% CI, 21.8%-24.1%) vs 28.1% (27.4%-28.7%) (P < .001). Patients with cancer had an adjusted odds ratio for hospital mortality of 1.09 (95% CI, 1.00-1.19). By 6 months, mortality in the cancer group was higher than that in the noncancer group at 31.3% compared with 28.2% (P < .001). Four years after ICU admission, mortality for those with and without cancer was 60.9% vs 39.7% (P < .001) respectively.
Conclusions and relevance: Cancer is a common diagnosis among surgical ICU patients and this study suggests that initial outcomes compare favorably with those of ICU patients with other conditions. Consideration that a diagnosis of cancer should not preclude admission to the ICU in patients with surgical disease is suggested.
Conflict of interest statement
Figures
Similar articles
-
Factors associated with intensive care admission in patients with lung cancer: a population-based observational study of 26, 731 patients.BMC Pulm Med. 2020 Feb 7;20(1):36. doi: 10.1186/s12890-020-1071-8. BMC Pulm Med. 2020. PMID: 32033549 Free PMC article.
-
Incidence, Risk Factors, and Attributable Mortality of Secondary Infections in the Intensive Care Unit After Admission for Sepsis.JAMA. 2016 Apr 12;315(14):1469-79. doi: 10.1001/jama.2016.2691. JAMA. 2016. PMID: 26975785
-
Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy.JAMA. 2020 Apr 28;323(16):1574-1581. doi: 10.1001/jama.2020.5394. JAMA. 2020. PMID: 32250385 Free PMC article.
-
Outcomes and prognostic factors in patients with haematological malignancy admitted to a specialist cancer intensive care unit: a 5 yr study.Br J Anaesth. 2012 Mar;108(3):452-9. doi: 10.1093/bja/aer449. Epub 2012 Jan 31. Br J Anaesth. 2012. PMID: 22298243 Review.
-
One for the ages: optimizing geriatric care in the intensive care unit.Trauma Surg Acute Care Open. 2025 Apr 14;10(Suppl 1):e001785. doi: 10.1136/tsaco-2025-001785. eCollection 2025. Trauma Surg Acute Care Open. 2025. PMID: 40521176 Free PMC article. Review.
Cited by
-
One-year Mortality of Cancer Patients with an Unplanned ICU Admission: A Cohort Analysis Between 2008 and 2017 in the Netherlands.J Intensive Care Med. 2022 Sep;37(9):1165-1173. doi: 10.1177/08850666211054369. Epub 2021 Nov 17. J Intensive Care Med. 2022. PMID: 34787492 Free PMC article.
-
The effect of the underlying malignancy on short- and medium-term survival of critically ill patients admitted to the intensive care unit: a retrospective analysis based on propensity score matching.BMC Cancer. 2021 Apr 15;21(1):417. doi: 10.1186/s12885-021-08152-5. BMC Cancer. 2021. PMID: 33858357 Free PMC article.
-
Outcome of glioblastoma patients after intensive care unit admission with invasive mechanical ventilation: a multicenter analysis.J Neurooncol. 2023 Aug;164(1):249-256. doi: 10.1007/s11060-023-04403-6. Epub 2023 Aug 2. J Neurooncol. 2023. PMID: 37530945 Free PMC article.
-
Etiologies and Outcome of Patients with Solid Tumors Admitted to ICU with Acute Respiratory Failure: A Secondary Analysis of the EFRAIM Study.Respir Care. 2023 Jun;68(6):740-748. doi: 10.4187/respcare.10604. Epub 2023 Apr 18. Respir Care. 2023. PMID: 37072164 Free PMC article.
-
A clinically applicable prediction model for the risk of in-hospital mortality in solid cancer patients admitted to intensive care units with sepsis.J Cancer Res Clin Oncol. 2023 Aug;149(10):7175-7185. doi: 10.1007/s00432-023-04661-x. Epub 2023 Mar 8. J Cancer Res Clin Oncol. 2023. PMID: 36884120 Free PMC article.
References
-
- Puxty K, McLoone P, Quasim T, Sloan B, Kinsella J, Morrison DS. Risk of critical illness among patients with solid cancers: a population-based observational study. JAMA Oncol. 2015;1(8):1078-1085. - PubMed
-
- Cancer incidence in five continents Vol. IX; IARC Scientific Publication, No. 160. Anticancer Res. 2009;29(11).
-
- Garrouste-Orgeas M, Montuclard L, Timsit JF, et al. ; French ADMISSIONREA Study Group . Predictors of intensive care unit refusal in French intensive care units: a multiple-center study. Crit Care Med. 2005;33(4):750-755. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
