

Patient-Reported Symptoms Over 48 Weeks Among Participants in Randomized, Double-Blind, Phase III Non-inferiority Trials of Adults with HIV on Co-formulated Bictegravir, Emtricitabine, and Tenofovir Alafenamide versus Co-formulated Abacavir, Dolutegravir, and Lamivudine
- PMID: 29956087
- PMCID: PMC6132439
- DOI: 10.1007/s40271-018-0322-8
Patient-Reported Symptoms Over 48 Weeks Among Participants in Randomized, Double-Blind, Phase III Non-inferiority Trials of Adults with HIV on Co-formulated Bictegravir, Emtricitabine, and Tenofovir Alafenamide versus Co-formulated Abacavir, Dolutegravir, and Lamivudine
Abstract
Background: Integrase strand transfer inhibitors (INSTIs) are recommended for first-line antiretroviral therapy in combination with two nucleos(t)ide reverse transcriptase inhibitors. Co-formulated bictegravir, emtricitabine, and tenofovir alafenamide (B/F/TAF), a novel, INSTI-based regimen, is currently approved in the US and EU for the treatment of HIV-1 infection and recommended as first-line treatment in current guidelines. In our current analysis, we aimed to determine changes in patient-reported symptoms over time among HIV-1-infected adults who initiated or switched to B/F/TAF versus another INSTI-based regimen, co-formulated abacavir, dolutegravir, and lamivudine (ABC/DTG/3TC).
Methods: A planned secondary analysis of patient-reported outcomes was conducted for two double-blind, randomized, phase III studies in HIV-1-infected adults comparing B/F/TAF with ABC/DTG/3TC: one in treatment-naïve individuals (GS-US-380-1489, ClinicalTrials.gov NCT02607930) and the other in virologically suppressed participants (GS-US-380-1844, ClinicalTrials.gov NCT02603120). In both studies, the HIV symptoms distress module (HIV-SI) was administered at baseline (BL) and weeks 4, 12, and 48. Responses to each of the 20 items were dichotomized as bothersome or not bothersome. Treatment differences were assessed using unadjusted and adjusted logistic regression models (adjusted for BL HIV-SI count, age, sex, BL Veterans Aging Cohort Study [VACS] Index, medical history of serious mental illness, BL Short Form [SF]-36 Physical Component Summary [PCS], BL SF-36 Mental Component Summary [MCS], and, for virologically suppressed participants only, years since HIV diagnosis). We conducted longitudinal modeling of bothersome symptoms using a generalized mixed model including treatment, time, time-by-treatment, and additional covariates from the adjusted logistic regression model as described above. The Pittsburgh Sleep Quality Index (PSQI) was administered at the same frequency as the HIV-SI, and the total score was dichotomized as good or poor sleep quality. Similar models to those used for HIV-SI were applied, using BL sleep quality and BL SF-36 MCS as covariates. Statistical significance was assessed using p < 0.05.
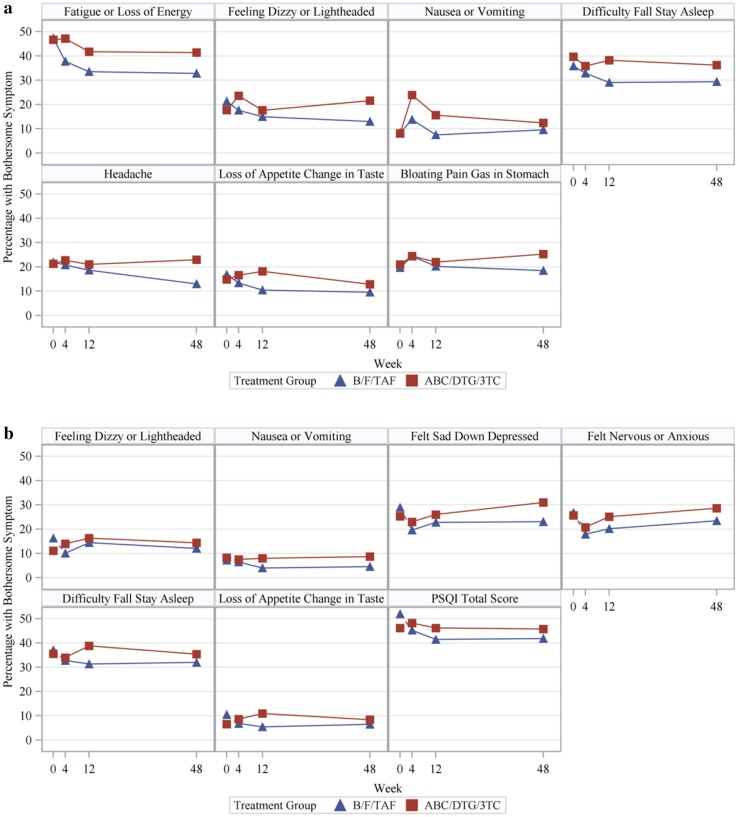
Results: Across both studies, bothersome symptoms were reported by fewer participants on B/F/TAF than those on ABC/DTG/3TC. In treatment-naïve adults, fatigue/loss of energy, nausea/vomiting, dizzy/lightheadedness, and difficulty sleeping were reported significantly less with B/F/TAF at two or more time points. Fatigue and nausea were also significantly less common for those receiving B/F/TAF in longitudinal models. In virologically suppressed participants, nausea/vomiting, sad/down/depressed, nervous/anxious, and poor sleep quality (from the PSQI) were reported significantly less with B/F/TAF at two or more time points, as well as in longitudinal models.
Conclusions: B/F/TAF was associated with lower prevalence of bothersome symptoms than ABC/DTG/3TC in both treatment-naïve and virologically suppressed adults.
Conflict of interest statement
Potential Conflicts of Interest and Sources of Funding: Dr Wohl has served on advisory boards for Gilead and Janssen, and has received research grants to the University of North Carolina from Gilead. Dr Clarke has served on advisory boards for GSK and Gilead, and has received conference attendance support from Janssen, BMS and Gilead, and received a speaker fee from Gilead. Dr Maggiolo has served on advisory boards for Abbvie, Bristol-Myers Squibb, Gilead, GlaxoSmithKline, Tibotec, and has received research grants to ASST Papa Giovanni XXIII from Abbvie, Bristol-Myers Squibb, Gilead, GlaxoSmithKline, and Janssen. Drs Garner, Laouri, Martin, and Quirk are employees of Gilead Sciences and hold stock options in the company.
This study was funded by Gilead Sciences. This study was conducted in accordance with the Declaration of Helsinki. The protocol was reviewed and approved by central or site-specific institutional review boards or ethics committees covering all participating sites. All participants provided written informed consent.
Figures
References
-
- European AIDS Clinical Society. Guidelines. Version 9.0. October 2017. Brussels: European AIDS Clinical Society, 2017. www.eacsociety.org/files/guidelines_9.0-english.pdf. Accessed 30 May 2018.
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents: U. S. Department of Health and Human Services, Washington D.C., USA. https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf. Last Updated 27 March 2018. Accessed 30 May 2018.
-
- Blanco J, Montaner JSG, Matconi VC, et al. Lower prevalence of drug resistance mutations at first-line virological failure to first-line therapy with atripla vs. tenpfovir + emtricitabine/lamivudine + efavirenz administered on a multiple tablet therapy. AIDS. 2015;28:2531–2539. doi: 10.1097/QAD.0000000000000424. - DOI - PubMed
-
- Elliot E, Chirwa M, Boffito M. How recent findings on the pharmacokinetics and pharmacodynamics of integrase inhibitors can inform clinical use. Curr Opin Infect Dis. 2017;30:58–73. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
