

Genome Editing of Induced Pluripotent Stem Cells to Decipher Cardiac Channelopathy Variant
- PMID: 29957233
- PMCID: PMC6050025
- DOI: 10.1016/j.jacc.2018.04.041
Genome Editing of Induced Pluripotent Stem Cells to Decipher Cardiac Channelopathy Variant
Abstract
Background: The long QT syndrome (LQTS) is an arrhythmogenic disorder of QT interval prolongation that predisposes patients to life-threatening ventricular arrhythmias such as Torsades de pointes and sudden cardiac death. Clinical genetic testing has emerged as the standard of care to identify genetic variants in patients suspected of having LQTS. However, these results are often confounded by the discovery of variants of uncertain significance (VUS), for which there is insufficient evidence of pathogenicity.
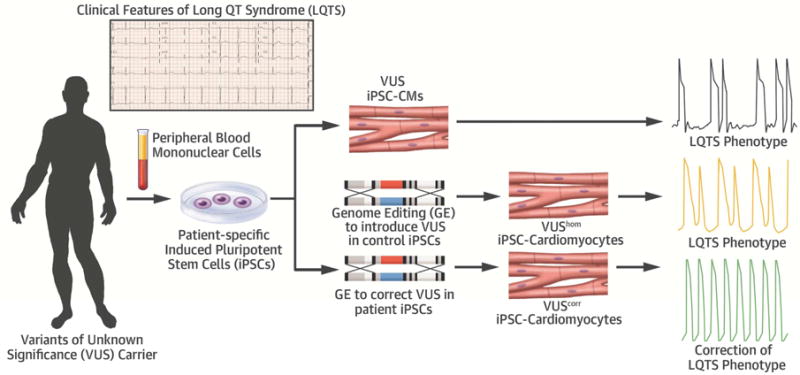
Objectives: The purpose of this study was to demonstrate that genome editing of patient-specific induced pluripotent stem cells (iPSCs) can be a valuable approach to delineate the pathogenicity of VUS in cardiac channelopathy.
Methods: Peripheral blood mononuclear cells were isolated from a carrier with a novel missense variant (T983I) in the KCNH2 (LQT2) gene and an unrelated healthy control subject. iPSCs were generated using an integration-free Sendai virus and differentiated to iPSC-derived cardiomyocytes (CMs).
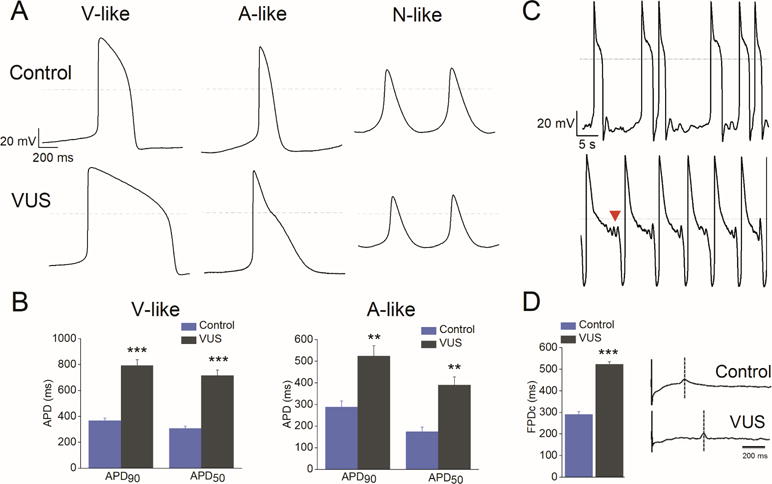
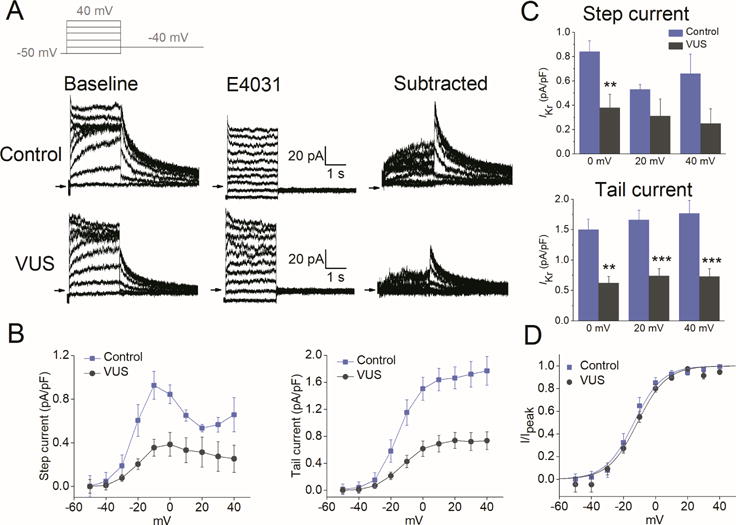
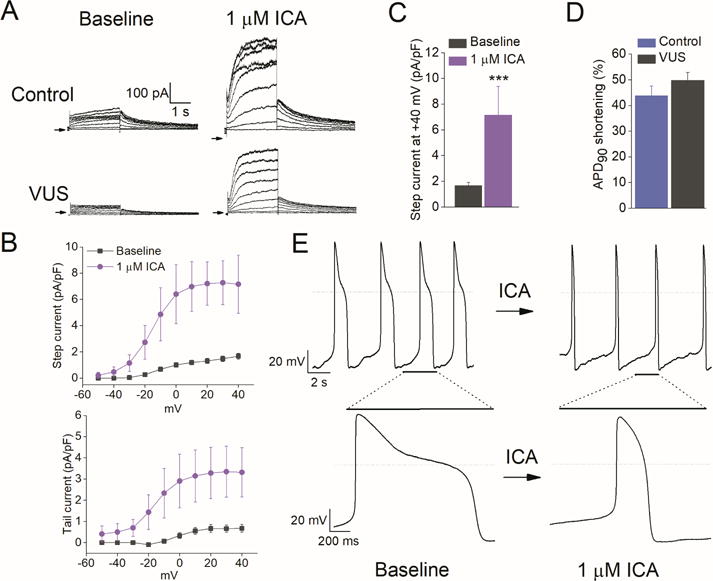
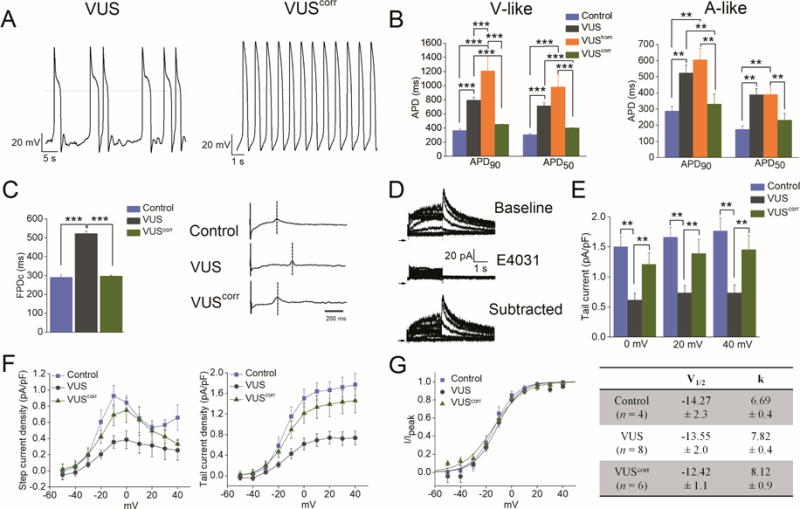
Results: Whole-cell patch clamp recordings revealed significant prolongation of the action potential duration (APD) and reduced rapidly activating delayed rectifier K+ current (IKr) density in VUS iPSC-CMs compared with healthy control iPSC-CMs. ICA-105574, a potent IKr activator, enhanced IKr magnitude and restored normal action potential duration in VUS iPSC-CMs. Notably, VUS iPSC-CMs exhibited greater propensity to proarrhythmia than healthy control cells in response to high-risk torsadogenic drugs (dofetilide, ibutilide, and azimilide), suggesting a compromised repolarization reserve. Finally, the selective correction of the causal variant in iPSC-CMs using CRISPR/Cas9 gene editing (isogenic control) normalized the aberrant cellular phenotype, whereas the introduction of the homozygous variant in healthy control cells recapitulated hallmark features of the LQTS disorder.
Conclusions: The results suggest that the KCNH2T983I VUS may be classified as potentially pathogenic.
Keywords: arrhythmia; genome editing; induced pluripotent stem cells; long QT syndrome; variant of uncertain significance.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures



Comment in
-
CRISPRed Cardiomyocytes to Decrypt Variants of Uncertain Significance.J Am Coll Cardiol. 2018 Jul 3;72(1):76-78. doi: 10.1016/j.jacc.2018.05.004. J Am Coll Cardiol. 2018. PMID: 29957234 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
