

Diagnostic Value of Diffusion-Weighted Imaging and Apparent Diffusion Coefficient in Assessment of the Activity of Crohn Disease: 1.5 or 3 T
- PMID: 29958199
- PMCID: PMC6296832
- DOI: 10.1097/RCT.0000000000000754
Diagnostic Value of Diffusion-Weighted Imaging and Apparent Diffusion Coefficient in Assessment of the Activity of Crohn Disease: 1.5 or 3 T
Abstract
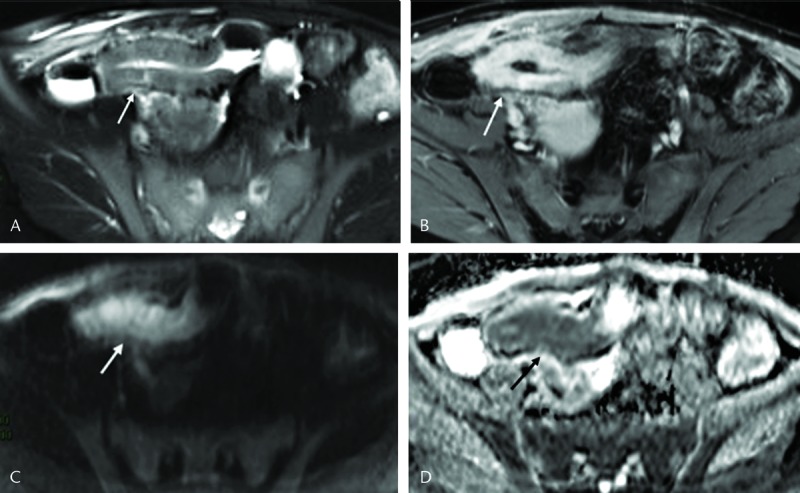
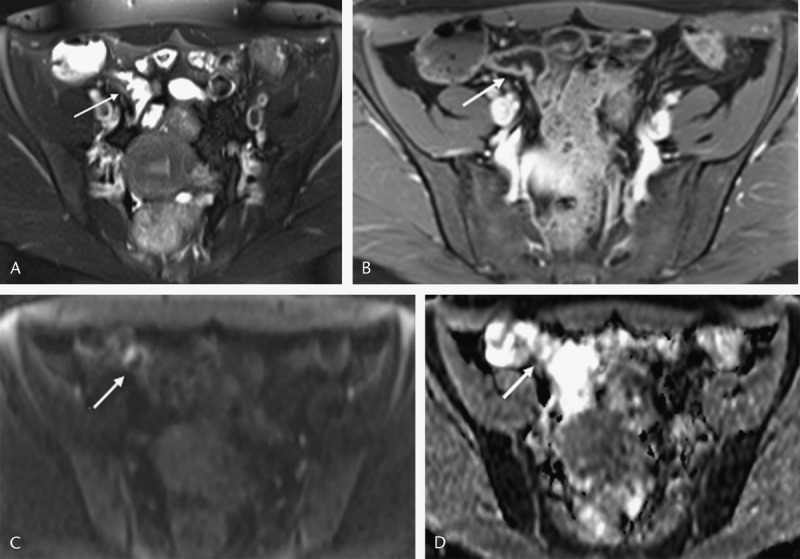
Objective: The objective of this study is to evaluate the role of diffusion-weighted imaging (DWI) in assessment of the activity of Crohn disease (CD) and to explore differences between DWI in 3 T and 1.5 T.
Methods: Postcontrast magnetic resonance enterography with DWI of 72 patients with pathological proof of CD was retrospectively evaluated for restricted diffusion qualitatively and quantitavely in 3 T (n = 40) and 1.5 T (n = 32). Magnetic resonance activity score of 7 or higher was used as reference of activity.
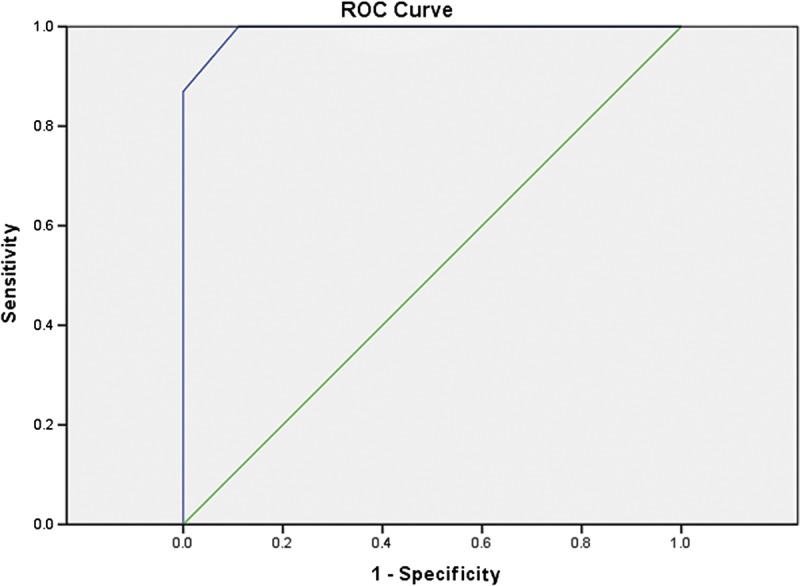
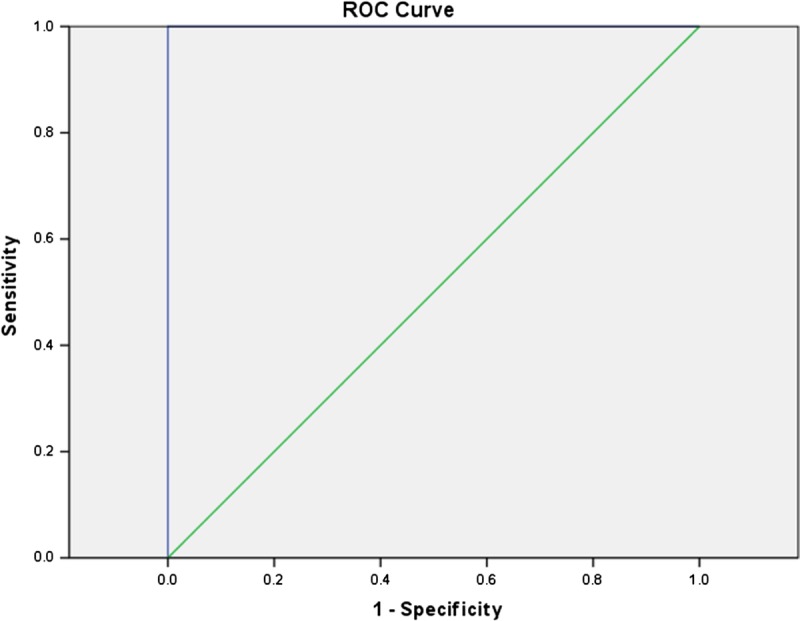
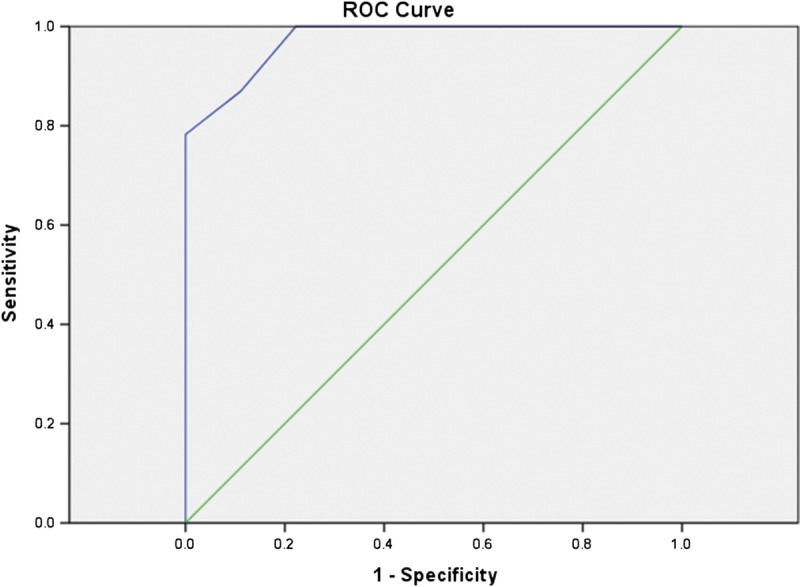
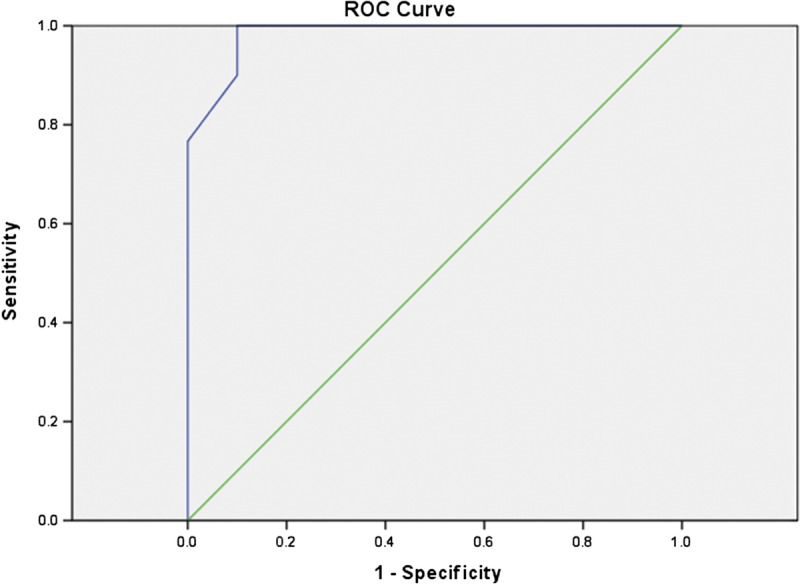
Results: Fifty-five patients had active lesions. Diffusion-weighted imaging hyperintensity showed sensitivity (100%, 100%) and specificity (88.89%, 100%) in 1.5/3 T for activity assessment. Mean ± SD apparent diffusion coefficient for active lesions was 1.21 ± 0.42 and 1.28 ± 0.59 × 10 mm/s in 1.5 and 3 T, respectively. The proposed cutoff values of 1.35 and 1.38 × 10 mm/s in 1.5 and 3 T, respectively, had sensitivity (80%, 93%), specificity (100%, 90%), accuracy (88%, 93%), and no significant difference in accuracy between 1.5/3 T (P = 0.48).
Conclusions: Diffusion-weighted imaging hypersensitivity and apparent diffusion coefficient values accurately assessed the activity of CD. No significant statistical difference in diagnostic accuracy was detected between 1.5 and 3 T.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
Similar articles
-
Value of diffusion-weighted imaging when added to magnetic resonance enterographic evaluation of Crohn disease in children.Pediatr Radiol. 2016 Jan;46(1):34-42. doi: 10.1007/s00247-015-3438-1. Epub 2015 Aug 4. Pediatr Radiol. 2016. PMID: 26238966
-
Diffusion kurtosis MRI versus conventional diffusion-weighted imaging for evaluating inflammatory activity in Crohn's disease.J Magn Reson Imaging. 2018 Mar;47(3):702-709. doi: 10.1002/jmri.25768. Epub 2017 Jun 3. J Magn Reson Imaging. 2018. PMID: 28577319
-
MR Enterography for the Evaluation of Small-Bowel Inflammation in Crohn Disease by Using Diffusion-weighted Imaging without Intravenous Contrast Material: A Prospective Noninferiority Study.Radiology. 2016 Mar;278(3):762-72. doi: 10.1148/radiol.2015150809. Epub 2015 Sep 8. Radiology. 2016. PMID: 26348103
-
Diffusion-weighted MRI in Crohn's disease: Current status and recommendations.J Magn Reson Imaging. 2016 Dec;44(6):1381-1396. doi: 10.1002/jmri.25325. Epub 2016 Jun 1. J Magn Reson Imaging. 2016. PMID: 27249184 Review.
-
Diffusion-weighted imaging in pediatric body magnetic resonance imaging.Pediatr Radiol. 2016 May;46(6):847-57. doi: 10.1007/s00247-016-3573-3. Epub 2016 May 26. Pediatr Radiol. 2016. PMID: 27229502 Review.
Cited by
-
Role of abbreviated non-contrast-enhanced MR-enterography in the evaluation of Crohn's disease activity and complications as an alternative for full protocol contrast-enhanced study: A systematic review and meta-analysis.Res Diagn Interv Imaging. 2023 Apr 28;6:100030. doi: 10.1016/j.redii.2023.100030. eCollection 2023 Jun. Res Diagn Interv Imaging. 2023. PMID: 39077544 Free PMC article.
-
The onset of ulcerative colitis upon Helicobacter pylori eradication in a 72-year-old woman: report of a rare case with a 3-year follow-up.BMC Gastroenterol. 2021 Jul 31;21(1):303. doi: 10.1186/s12876-021-01876-5. BMC Gastroenterol. 2021. PMID: 34332529 Free PMC article.
-
A polymeric diet rich in transforming growth factor beta 2 does not reduce inflammation in chronic 2,4,6-trinitrobenzene sulfonic acid colitis in pre-pubertal rats.BMC Gastroenterol. 2020 Dec 10;20(1):416. doi: 10.1186/s12876-020-01574-8. BMC Gastroenterol. 2020. PMID: 33302890 Free PMC article.
-
An Unexpected Gastric Subepithelial Mass.Oman Med J. 2021 Mar 31;36(2):e252. doi: 10.5001/omj.2021.36. eCollection 2021 Mar. Oman Med J. 2021. PMID: 33959382 Free PMC article. No abstract available.
-
Assessment of lacrimal glands in thyroid eye disease with diffusion-weighted magnetic resonance imaging.Pol J Radiol. 2019 Mar 8;84:e142-e146. doi: 10.5114/pjr.2019.84096. eCollection 2019. Pol J Radiol. 2019. PMID: 31019608 Free PMC article.
References
-
- Peyrin-Biroulet L, Loftus EV, Jr, Colombel JF, et al. The natural history of adult Crohn's disease in population-based cohorts. Am J Gastroenterol. 2010;105:289–297. - PubMed
-
- Dignass A, Van Assche G, Lindsay JO, et al. The second European evidence-based Consensus on the diagnosis and management of Crohn's disease: current management. J Crohns Colitis. 2010;4:28–62. - PubMed
-
- Sandborn WJ, Feagan BG, Hanauer SB, et al. A review of activity indices and efficacy endpoints for clinical trials of medical therapy in adults with Crohn's disease. Gastroenterology. 2002;122:512–530. - PubMed
-
- Daperno M, D'Haens G, Van Assche G, et al. Development and validation of a new, simplified endoscopic activity score for Crohn's disease: the SES-CD. Gastrointest Endosc. 2004;60:505–512. - PubMed
-
- Bourreille A, Ignjatovic A, Aabakken L, et al. Role of small-bowel endoscopy in the management of patients with inflammatory bowel disease: an international OMED-ECCO consensus. Endoscopy. 2009;41:618–637. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
