

Low-dose cytarabine to prevent myeloid leukemia in children with Down syndrome: TMD Prevention 2007 study
- PMID: 29959152
- PMCID: PMC6039662
- DOI: 10.1182/bloodadvances.2018018945
Low-dose cytarabine to prevent myeloid leukemia in children with Down syndrome: TMD Prevention 2007 study
Abstract
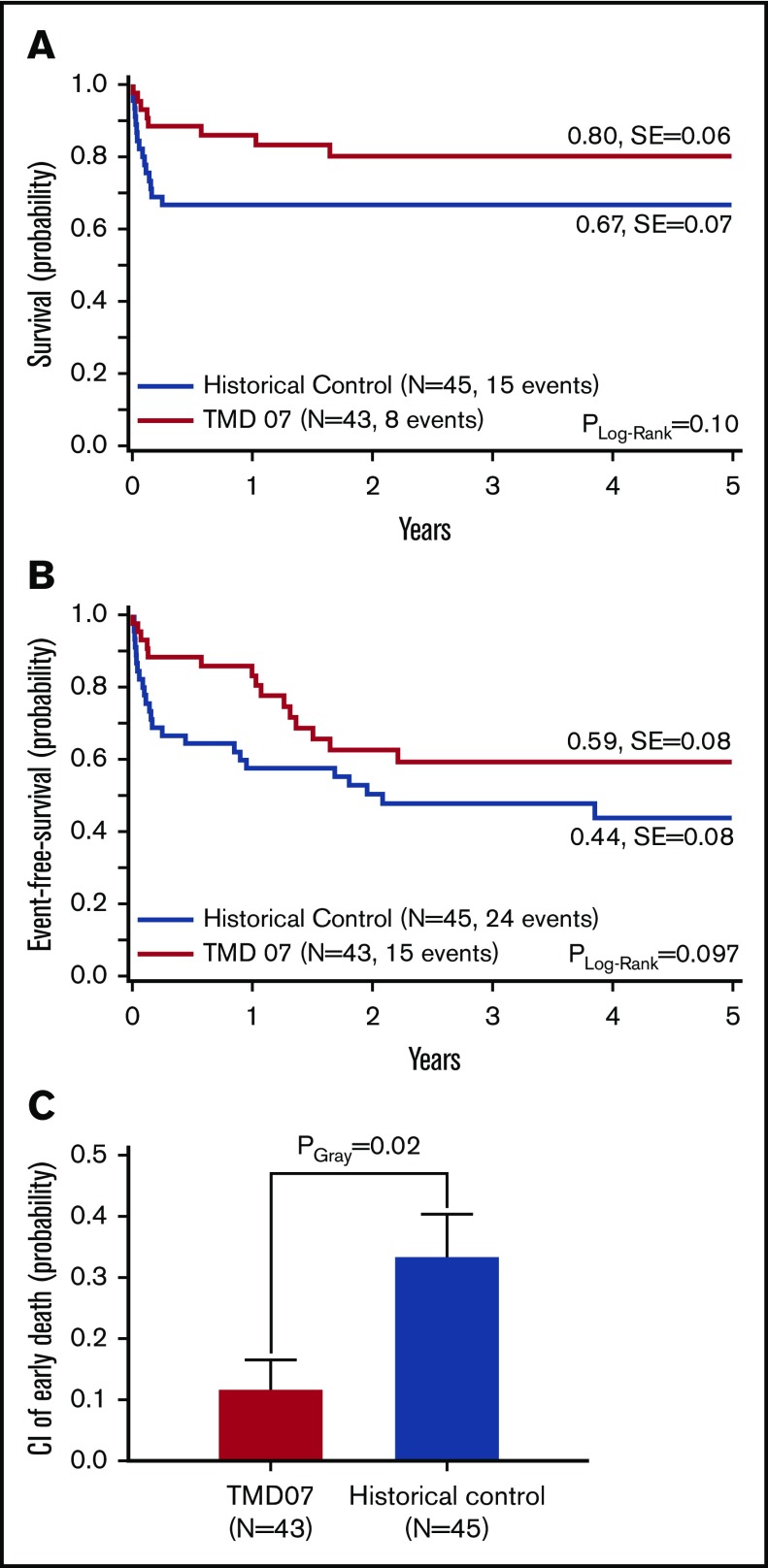
Approximately 5% to 10% of children with Down syndrome (DS) are diagnosed with transient myeloproliferative disorder (TMD). Approximately 20% of these patients die within 6 months (early death), and another 20% to 30% progress to myeloid leukemia (ML-DS) within their first 4 years of life. The aim of the multicenter, nonrandomized, historically controlled TMD Prevention 2007 trial was to evaluate the impact of low-dose cytarabine treatment on survival and prevention of ML-DS in patients with TMD. Patients received cytarabine (1.5 mg/kg for 7 days) in case of TMD-related symptoms at diagnosis (high white blood cell count, ascites, liver dysfunction, hydrops fetalis) or detection of minimal residual disease (MRD) 8 weeks after diagnosis. The 5-year probability of event-free and overall survival of 102 enrolled TMD patients was 72 ± 5% and 91 ± 3%, respectively. In patients eligible for treatment because of symptoms (n = 43), we observed a significantly lower cumulative incidence (CI) of early death as compared with symptomatic patients in the historical control (n = 45) (12 ± 5% vs 33 ± 7%, PGray = .02). None of the asymptomatic patients in the current study suffered early death. However, the treatment of symptomatic or MRD-positive patients did not result in a significantly lower CI of ML-DS (25 ± 7% [treated] vs 14 ± 7% [untreated], PGray = .34 [per protocol analysis]; historical control: 22 ± 4%, PGray = .55). Thus, low-dose cytarabine treatment helped to reduce TMD-related mortality when compared with the historical control but was insufficient to prevent progression to ML-DS. This trial was registered at EudraCT as #2006-002962-20.
© 2018 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: D.R. has consulting or advisory roles for Celgene, Pfizer, MSD, Astellas Pharma, BlueBirdBio, Amgen, Novartis, and Boehringer and receives research funding from Celgene. C.M.Z. has consulting or advisory roles for Pfizer, Daiichi Sankyo, Celgene, Novartis, Bristol-Myers Squibb, and Gilead Sciences and receives research funding from Karyopharm Therapeutics, Pfizer, Bristol-Myers Squibb, and GlaxoSmithKline. The remaining authors declare no competing financial interests.
Figures




References
-
- Pine SR, Guo Q, Yin C, Jayabose S, Druschel CM, Sandoval C. Incidence and clinical implications of GATA1 mutations in newborns with Down syndrome. Blood. 2007;110(6):2128-2131. - PubMed
-
- Langebrake C, Creutzig U, Reinhardt D. Immunophenotype of Down syndrome acute myeloid leukemia and transient myeloproliferative disease differs significantly from other diseases with morphologically identical or similar blasts. Klin Padiatr. 2005;217(3):126-134. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
