

Age-related differences in humoral and cellular immune responses after primary immunisation: indications for stratified vaccination schedules
- PMID: 29959387
- PMCID: PMC6026142
- DOI: 10.1038/s41598-018-28111-8
Age-related differences in humoral and cellular immune responses after primary immunisation: indications for stratified vaccination schedules
Abstract
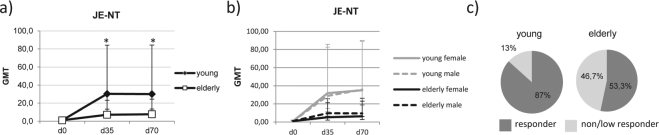
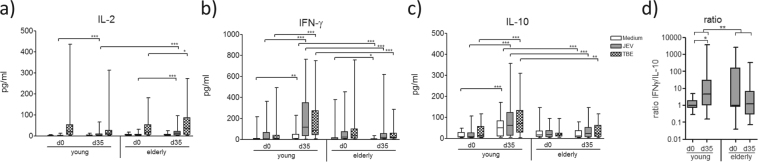
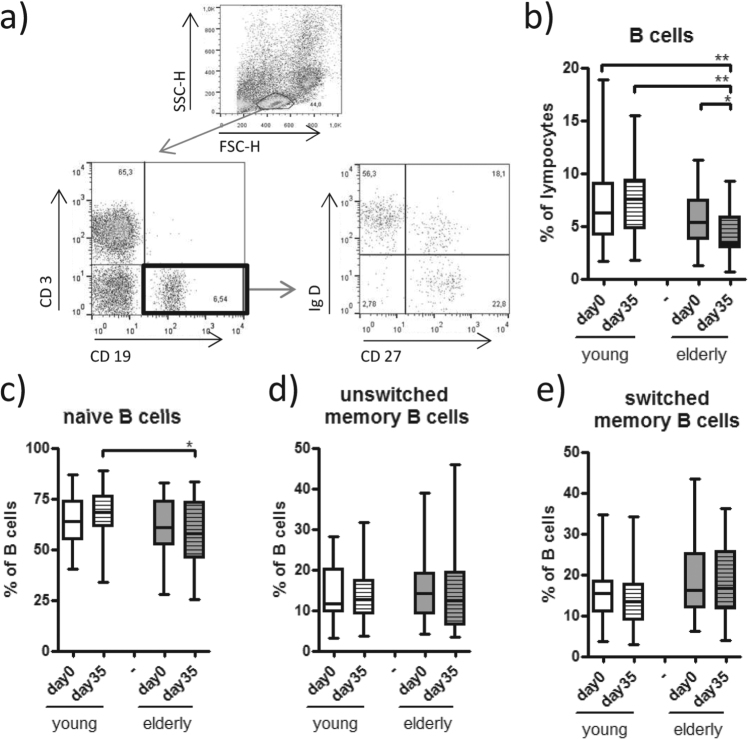
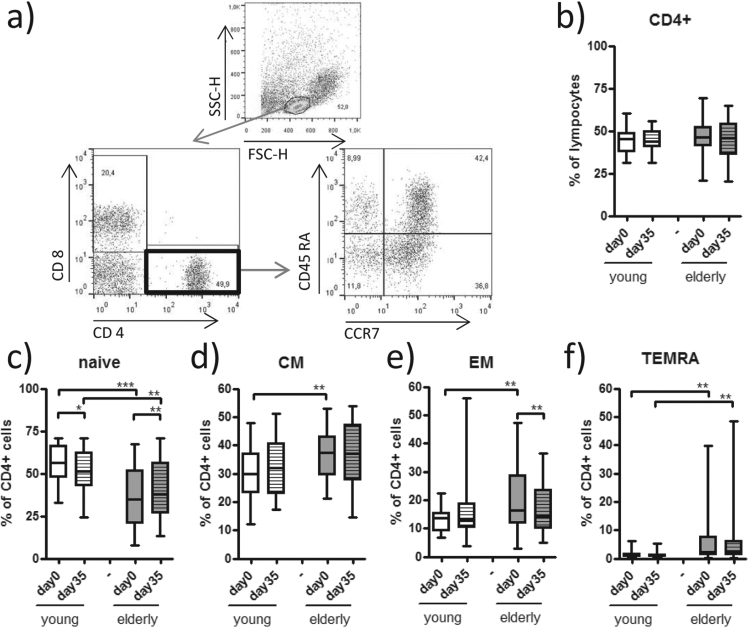
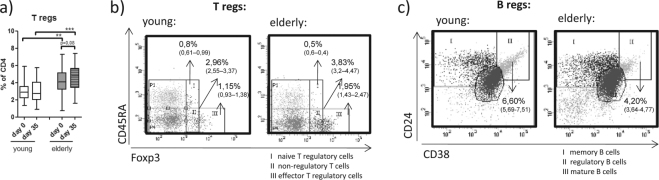
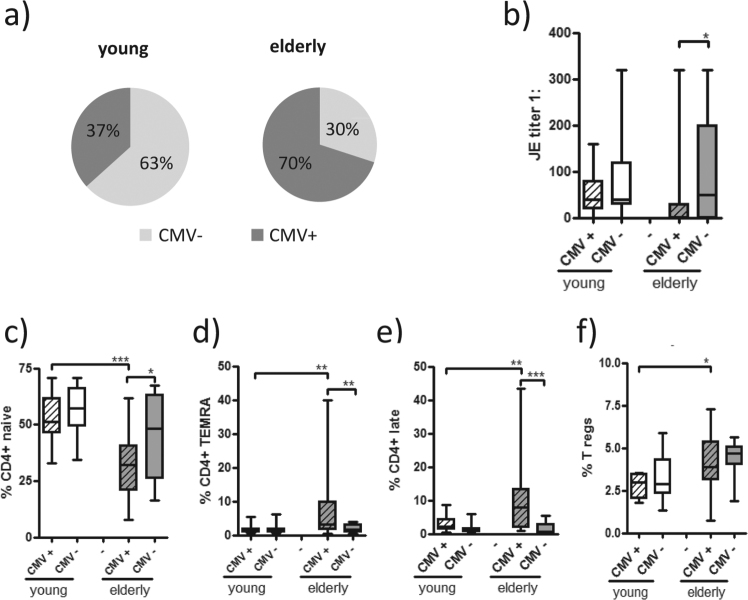
Immunosenescence is characterised by reduced B and T cell responses. Evidence shows that booster vaccinations are less effective in elderly people, but data on the efficacy of primary immunisation are sparse. We conducted a monocentric, open label, phase IV trial to compare immune responses to primary vaccinations using the inactivated, adjuvanted Japanese Encephalitis vaccine by 30 elderly people (mean 69, range 61-78 years) and 30 younger people (mean 24, range 18-30 years). Humoral and cellular immune responses were analysed in relation to age and cytomegalovirus (CMV) seropositivity. Vaccine-specific antibody titres were significantly lower in elderly participants and 47% of them were non- or low responders after the two doses of the vaccine neo-antigen. The reduced humoral immune responses in elderly people correlated with reduced cytokine production, such as interferon gamma (IFN-γ) in vitro, as well as higher frequencies of late-differentiated effector and effector memory T cells and T regulatory cells. These cellular changes and lower antibody titres were particularly prominent in CMV-seropositive elderly participants. If primary vaccination before the age of 60 is not possible, elderly patients may require different vaccination strategies to ensure sufficient long-lasting immunity, such as adapted or accelerated schedules and the use of different adjuvants.
Conflict of interest statement
UW declares that she and HK have been commissioned as expert witnesses by the Austrian government. We received financial support by Novartis (at this time holding the market/sales authorization of Ixiaro® in Austria) to purchase the vaccine for this study. For antigen restimulation, the JEV antigen was kindly provided by Dr Klade, formerly of Intercell and now Valneva and the TBE antigen strain Neudörfl was provided by Baxter now Pfizer.
Figures
References
-
- United Nations, D. o. E. a. S. A., Population Division. World Population Ageing, http://www.un.org/en/development/desa/population/theme/ageing/WPA2015.shtml (2015).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
