

Pre-, Perinatal, and Parental Predictors of Body Mass Index Trajectory Milestones
- PMID: 29960766
- PMCID: PMC6153023
- DOI: 10.1016/j.jpeds.2018.05.041
Pre-, Perinatal, and Parental Predictors of Body Mass Index Trajectory Milestones
Abstract
Objective: To assess associations of pre-, perinatal, and parental factors with age and magnitude at body mass index (BMI) peak and rebound.
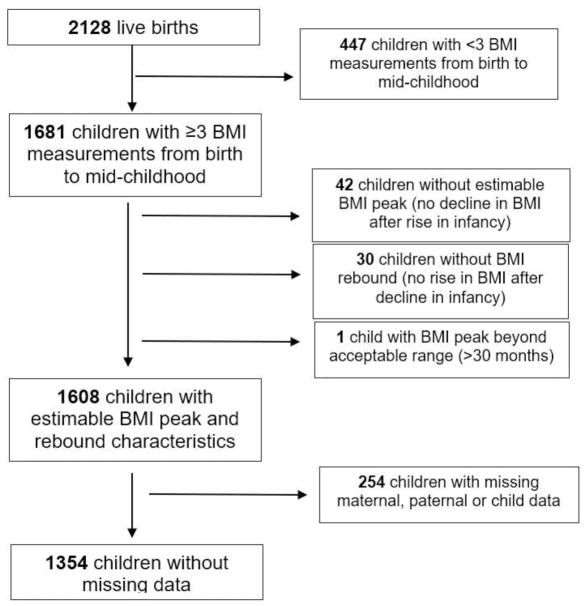
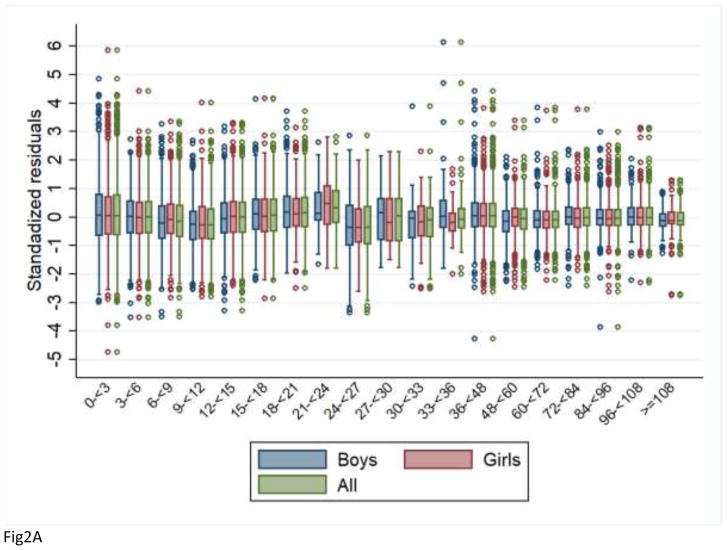
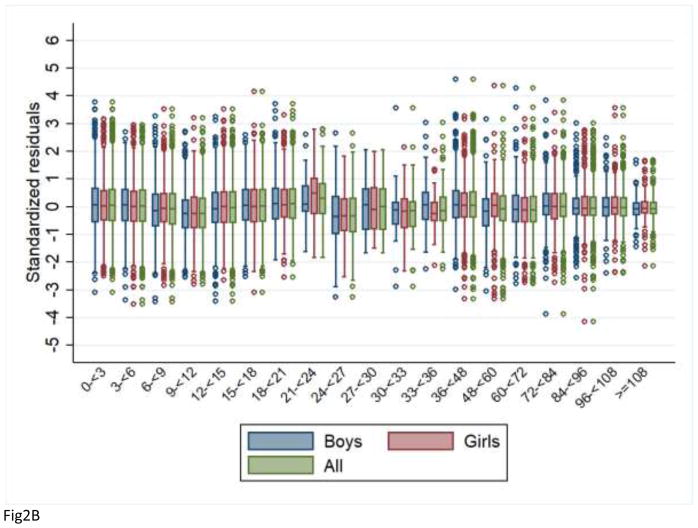
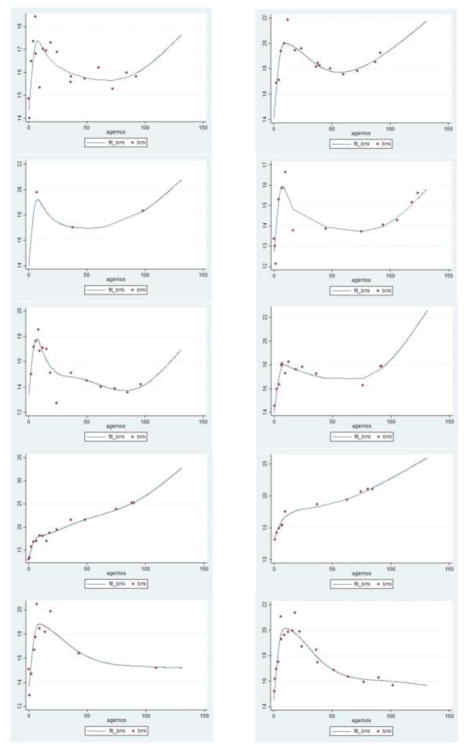
Study design: Among 1681 children with BMI data from birth to mid-childhood in Project Viva, we fitted individual BMI trajectories using mixed-effect models with natural cubic spline functions and estimated age and magnitude at peak in infancy and rebound in early childhood. We used stepwise multivariable regression to identify predictors of peak and rebound in the 1354 (63.6%) children with estimable trajectory milestones.
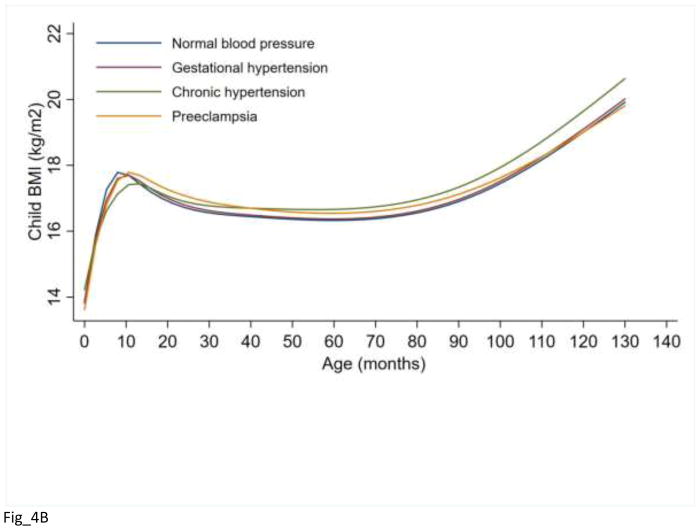
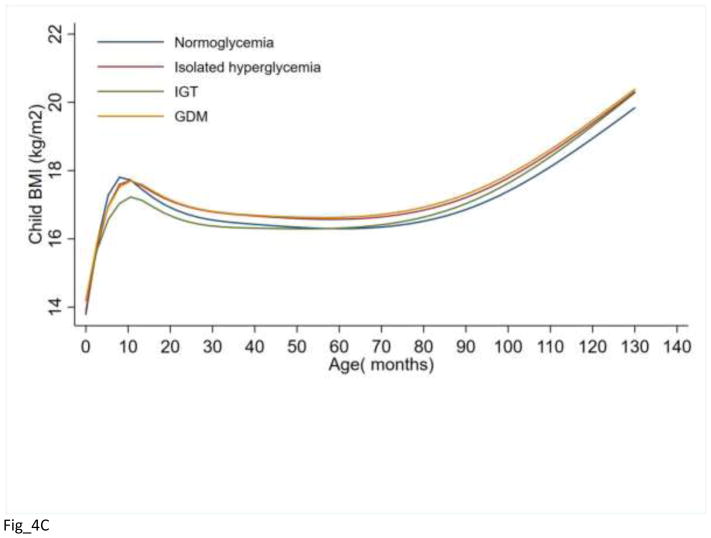
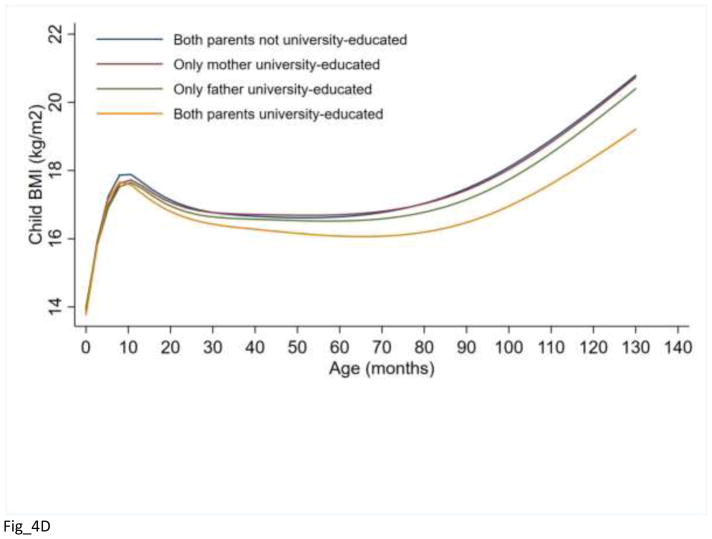
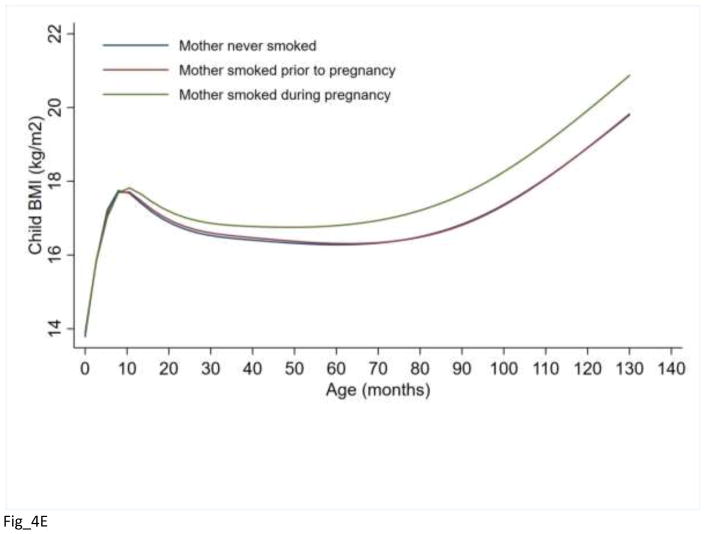
Results: The mean (SD) of age at BMI peak was 8.4 (2.7) months and at rebound was 59.8 (19.6) months, and the mean (SD) of magnitude at peak was 18.0 (1.4) kg/m2 and at rebound was 15.9 (1.2) kg/m2. Girls had a later age at peak, earlier age at rebound, and lower magnitudes at peak and rebound than boys. Maternal isolated hyperglycemia (vs normoglycemia: β 0.7 months [95% CI 0.2-1.2]) and pre-eclampsia (vs normal blood pressure: 1.6 months [0.8-2.4]) were associated with a later peak, and impaired glucose tolerance (vs normoglycemia: -0.5 kg/m2 [-0.9, -0.1]) was associated with a lower magnitude at peak. Greater maternal first-trimester weight gain, smoking during pregnancy, no breastfeeding, parental obesity, and no university education were associated with greater BMI at rebound.
Conclusions: We have identified modifiable prenatal and parental predictors of BMI peak in infancy and rebound in childhood. Early-life interventions that address these factors may be effective in changing BMI peak and rebound and potentially preventing later obesity.
Keywords: body mass index peak; body mass index rebound; lifecourse epidemiology; predictors.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
The other authors declare no conflicts of interest.
Figures

Similar articles
-
Patterns of body mass index milestones in early life and cardiometabolic risk in early adolescence.Int J Epidemiol. 2019 Feb 1;48(1):157-167. doi: 10.1093/ije/dyy286. Int J Epidemiol. 2019. PMID: 30624710 Free PMC article.
-
Childhood body mass index trajectories: modeling, characterizing, pairwise correlations and socio-demographic predictors of trajectory characteristics.BMC Med Res Methodol. 2012 Mar 29;12:38. doi: 10.1186/1471-2288-12-38. BMC Med Res Methodol. 2012. PMID: 22458308 Free PMC article.
-
Infant body mass index peak and early childhood cardio-metabolic risk markers in a multi-ethnic Asian birth cohort.Int J Epidemiol. 2017 Apr 1;46(2):513-525. doi: 10.1093/ije/dyw232. Int J Epidemiol. 2017. PMID: 27649801 Free PMC article.
-
Early adiposity rebound: predictors and outcomes.Ital J Pediatr. 2024 May 15;50(1):98. doi: 10.1186/s13052-024-01671-4. Ital J Pediatr. 2024. PMID: 38750561 Free PMC article. Review.
-
Offspring body size and metabolic profile - effects of lifestyle intervention in obese pregnant women.Dan Med J. 2014 Jul;61(7):B4893. Dan Med J. 2014. PMID: 25123127 Review.
Cited by
-
Early-Life Exposures and Risk of Diabetes Mellitus and Obesity.Curr Diab Rep. 2018 Aug 29;18(10):89. doi: 10.1007/s11892-018-1050-0. Curr Diab Rep. 2018. PMID: 30159823 Review.
-
Associations of cord blood leukocyte telomere length with adiposity growth from infancy to adolescence.Pediatr Obes. 2023 Jan;18(1):e12977. doi: 10.1111/ijpo.12977. Epub 2022 Sep 9. Pediatr Obes. 2023. PMID: 36085441 Free PMC article.
-
Patterns of body mass index milestones in early life and cardiometabolic risk in early adolescence.Int J Epidemiol. 2019 Feb 1;48(1):157-167. doi: 10.1093/ije/dyy286. Int J Epidemiol. 2019. PMID: 30624710 Free PMC article.
-
Associations of Neighborhood Opportunity and Social Vulnerability With Trajectories of Childhood Body Mass Index and Obesity Among US Children.JAMA Netw Open. 2022 Dec 1;5(12):e2247957. doi: 10.1001/jamanetworkopen.2022.47957. JAMA Netw Open. 2022. PMID: 36547983 Free PMC article.
-
Breastfeeding is associated with reduced risks of central obesity and hypertension in young school-aged children: a large, population-based study.Int Breastfeed J. 2023 Sep 11;18(1):52. doi: 10.1186/s13006-023-00581-1. Int Breastfeed J. 2023. PMID: 37697319 Free PMC article.
References
-
- Krebs NF, Jacobson MS. Prevention of pediatric overweight and obesity. Pediatrics. 2003 Aug;112:424–30. - PubMed
-
- U. S. Preventive Services Task Force. Screening for obesity in children and adolescents: Us preventive services task force recommendation statement. JAMA. 2017;317:2417–26. - PubMed
-
- Wen X, Kleinman K, Gillman MW, Rifas-Shiman SL, Taveras EM. Childhood body mass index trajectories: modeling, characterizing, pairwise correlations and socio-demographic predictors of trajectory characteristics. BMC Med Res Methodol. 2012 Mar 29;12:38. doi: 10.1186/471-2288-12-38. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
