

Presenting Signs and Symptoms do not Predict Aspiration Risk in Children
- PMID: 29960768
- PMCID: PMC6412137
- DOI: 10.1016/j.jpeds.2018.05.030
Presenting Signs and Symptoms do not Predict Aspiration Risk in Children
Abstract
Objectives: To determine if any presenting symptoms are associated with aspiration risk, and to evaluate the reliability of clinical feeding evaluation (CFE) in diagnosing aspiration compared with videofluoroscopic swallow study (VFSS).
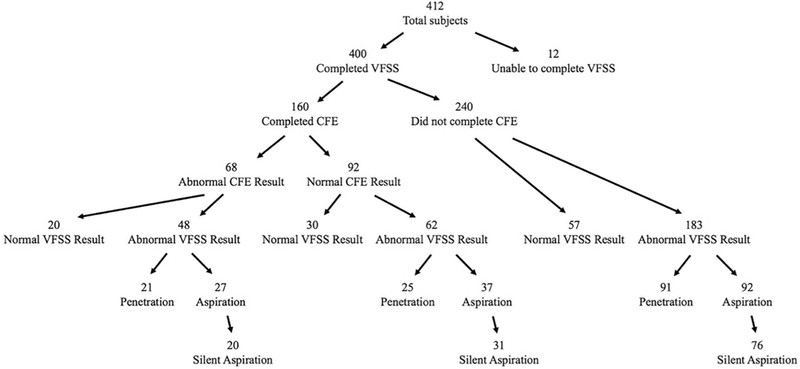
Study design: We retrospectively reviewed records of children under 2 years of age who had evaluation for oropharyngeal dysphagia by CFE and VFSS at Boston Children's Hospital and compared presenting symptoms, symptom timing, and CFE and VFSS results. We investigated the relationship between symptom presence and aspiration using the Fisher exact test and stepwise logistic regression with adjustment for comorbidities. CFE and VFSS results were compared using the McNemar test. Intervals from CFE to VFSS were compared using the Student t test.
Results: A total of 412 subjects with mean (±SD) age 8.9 ± 6.9 months were evaluated. No symptom, including timing relative to meals, predicted aspiration on VFSS. This lack of association between symptoms and VFSS results persisted even in the adjusted multivariate model. The sensitivity of CFE for predicting aspiration by VFSS was 44%. Patients with a reassuring CFE waited 28.2 ± 8.5 days longer for confirmatory VFSS compared with those with a concerning CFE (P < .05).
Conclusions: Presenting symptoms are varied in patients with aspiration and cannot be relied upon to determine which patients have aspiration on VFSS. The CFE does not have the sensitivity to consistently diagnose aspiration so a VFSS should be performed in persistently symptomatic patients.
Keywords: clinical feeding evaluation; oropharyngeal dysphagia; pediatrics; videofluoroscopic swallow study.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
It's hard to swallow-which test is best?J Pediatr. 2018 Oct;201:1-2. doi: 10.1016/j.jpeds.2018.07.104. J Pediatr. 2018. PMID: 30244723 No abstract available.
Similar articles
-
The Use of Cervical Auscultation to Predict Oropharyngeal Aspiration in Children: A Randomized Controlled Trial.Dysphagia. 2016 Dec;31(6):738-748. doi: 10.1007/s00455-016-9727-5. Epub 2016 Jul 11. Dysphagia. 2016. PMID: 27402004 Clinical Trial.
-
Oropharyngeal Dysphagia Is Strongly Correlated With Apparent Life-Threatening Events.J Pediatr Gastroenterol Nutr. 2017 Aug;65(2):168-172. doi: 10.1097/MPG.0000000000001439. J Pediatr Gastroenterol Nutr. 2017. PMID: 27741062 Free PMC article.
-
Infant Videofluoroscopic Swallow Study Testing, Swallowing Interventions, and Future Acute Respiratory Illness.Hosp Pediatr. 2016 Dec;6(12):707-713. doi: 10.1542/hpeds.2016-0049. Hosp Pediatr. 2016. PMID: 27879283
-
The modified barium swallow and the functional endoscopic evaluation of swallowing.Otolaryngol Clin North Am. 2013 Dec;46(6):1009-22. doi: 10.1016/j.otc.2013.08.001. Epub 2013 Oct 8. Otolaryngol Clin North Am. 2013. PMID: 24262956 Review.
-
Effect of Nasogastric Tube on Aspiration Risk: Results from 147 Patients with Dysphagia and Literature Review.Dysphagia. 2018 Dec;33(6):731-738. doi: 10.1007/s00455-018-9894-7. Epub 2018 Apr 4. Dysphagia. 2018. PMID: 29619559 Review.
Cited by
-
Videofluoroscopy compared with clinical feeding evaluation in children with suspected aspiration.Acta Paediatr. 2022 Jul;111(7):1441-1449. doi: 10.1111/apa.16338. Epub 2022 Apr 6. Acta Paediatr. 2022. PMID: 35316543 Free PMC article.
-
Outpatient Respiratory Management of Infants, Children, and Adolescents with Post-Prematurity Respiratory Disease: An Official American Thoracic Society Clinical Practice Guideline.Am J Respir Crit Care Med. 2021 Dec 15;204(12):e115-e133. doi: 10.1164/rccm.202110-2269ST. Am J Respir Crit Care Med. 2021. PMID: 34908518 Free PMC article.
-
Role of fiberoptic endoscopic evaluation of swallowing (FEES) in children with suspected dysphagia.J Pediatr (Rio J). 2024 Sep-Oct;100(5):476-482. doi: 10.1016/j.jped.2024.03.008. Epub 2024 Apr 26. J Pediatr (Rio J). 2024. PMID: 38679061 Free PMC article.
-
Breastfeeding in infants who aspirate may increase risk of pulmonary inflammation.Pediatr Pulmonol. 2024 Mar;59(3):600-608. doi: 10.1002/ppul.26788. Epub 2023 Dec 1. Pediatr Pulmonol. 2024. PMID: 38038162 Free PMC article.
-
Gastrointestinal Dysmotility and the Implications for Respiratory Disease.Curr Treat Options Pediatr. 2019 Jun;5(2):197-214. doi: 10.1007/s40746-019-00158-3. Epub 2019 Apr 26. Curr Treat Options Pediatr. 2019. PMID: 31134141 Free PMC article.
References
-
- Lefton-Greif MA, Carroll JL, Loughlin GM. Long-term follow-up of oropharyngeal dysphagia in children without apparent risk factors. Pediatric pulmonology 2006;41:1040–8. - PubMed
-
- Vaquero-Sosa E, Francisco-Gonzalez L, Bodas-Pinedo A, Urbasos-Garzon C, Ruiz-de-Leon-San-Juan A. Oropharyngeal dysphagia, an underestimated disorder in pediatrics. Rev Esp Enferm Dig 2015;107:113–5. - PubMed
-
- Durvasula VS, O’Neill AC, Richter GT. Oropharyngeal Dysphagia in children: mechanism, source, and management. Otolaryngologic clinics of North America 2014;47:691–720. - PubMed
-
- Weir K, McMahon S, Barry L, Masters IB, Chang AB. Clinical signs and symptoms of oropharyngeal aspiration and dysphagia in children. The European respiratory journal 2009;33:604–11. - PubMed
-
- Svystun O, Johannsen W, Persad R, Turner JM, Majaesic C, El-Hakim H. Dysphagia in healthy children: Characteristics and management of a consecutive cohort at a tertiary centre. International journal of pediatric otorhinolaryngology 2017;99:54–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
